The role of race and ethnicity in medicine is complex and requires a careful approach that considers the nuances of health equity. While acknowledging a patient’s ethnicity as part of the broader picture of social determinants of health (SDOH) can enhance accurate diagnoses and health assessments, the misuse or over-reliance on racial categorization has led to disparities in patient care and outcomes, particularly among minority populations.
Racial Disparities in Medical Access
An illustrative example of these complexities involves a clinical algorithm for kidney transplants. A 2019 study found that Black patients were less likely to be added to the national kidney transplant waitlist because an algorithm calculated them as healthier than they actually were. In response, a national task force recommended removing race from the scoring system, a change quickly adopted to improve racial equity in kidney care.
However, unintended consequences also arose. Removing race from the kidney function algorithm impacted access to chemotherapy, eligibility for clinical trials, and appropriate medicine dosing adjustments for Black patients. Research published in the Annals of Internal Medicine (available here and, see figure below) highlights how algorithms in healthcare, while designed to aid complex clinical decisions, can either help or hinder health equity, depending on their structure and application.

The Role of Algorithms in Healthcare
Healthcare algorithms, mathematical equations combining data points like age and sex, often shape clinical decisions, sometimes without patients or even clinicians being fully aware of their influence. These algorithms are frequently integrated into electronic medical records, providing quick guidance in disease diagnosis or treatment eligibility. Yet, there is limited oversight regarding how these algorithms impact health disparities.
A review of 63 studies by Penn Medicine found that there is no one-size-fits-all solution for correcting algorithmic biases. Some solutions include replacing race with more specific genetic or social variables and ensuring the data used to create these algorithms represents a diverse population. For example, modifying a lung cancer screening algorithm by removing race increased eligibility for Hispanic and Asian Americans but decreased it for Black patients. By making more precise adjustments based on individual risk factors, such as a patient’s genetic background or specific social factors, algorithms can be fine-tuned to serve a more equitable purpose.
Moving Toward Race-Aware Algorithms
According to a Health Affairs commentary from October 2023, a “race-aware” approach—focusing on precision medicine and increasing diversity in clinical trials—may be more effective than relying solely on race-based metrics. This approach is particularly relevant in interpreting diagnostic lab results, a fundamental step in clinical care. Medical tests, whether routine blood work, blood pressure measurements, or imaging, are the foundation for diagnosis and management.
The Need for Precision in Lab Result Interpretation
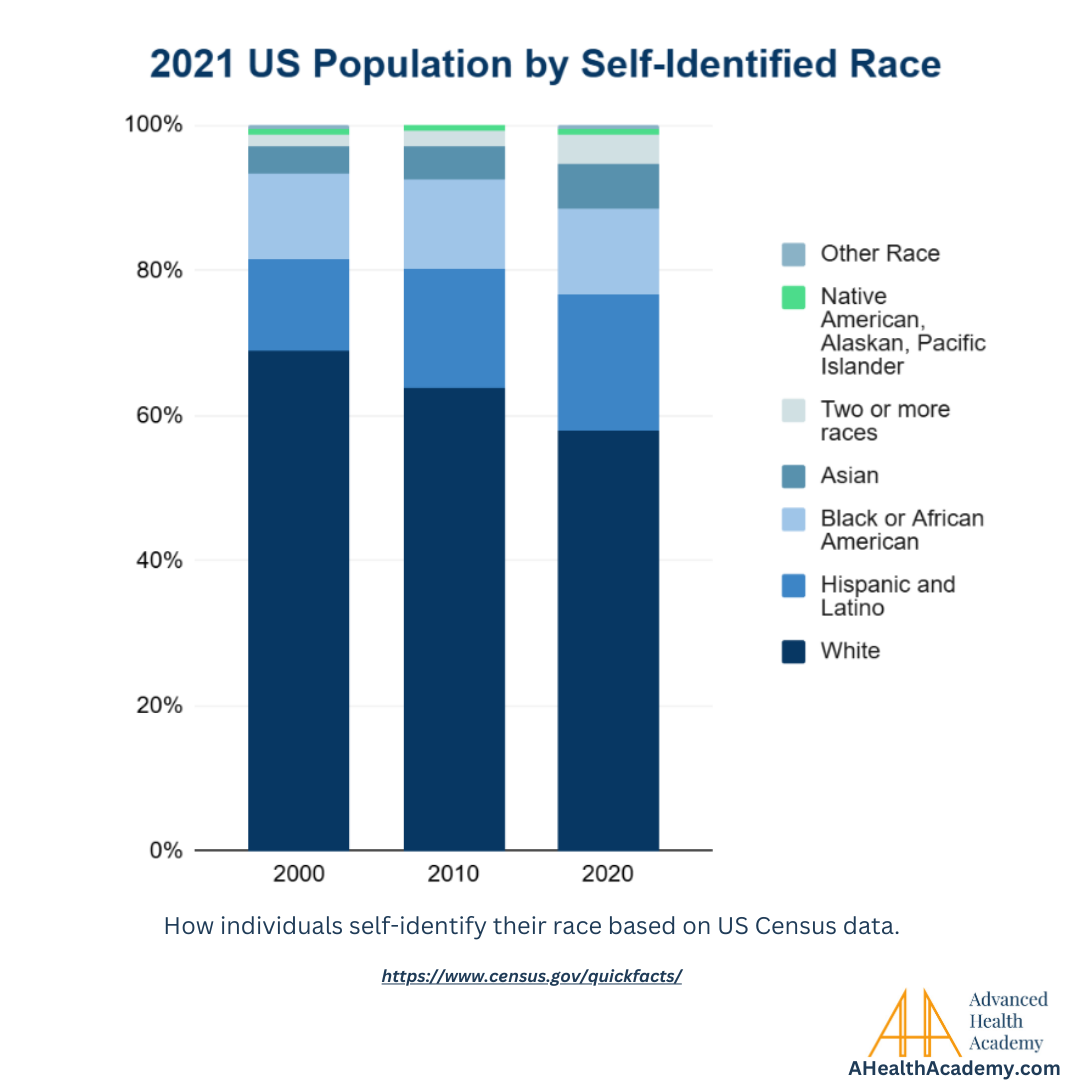
The United States is one of the most ethnically diverse countries, with over 40% of its population identifying outside the majority demographic, according to US census data. However, lab results are inconsistent with the latest scientific understanding of how race and ethnicity influence health assessments.
Take, for example, an adult patient born and raised in the U.S. by parents who emigrated from India. When looking at lab results, should the patient look at the normal ranges based on India or the U.S.? How is it possible to take both demographic profiles into account?
Research suggests that South Asians face a significantly higher risk of heart disease even at lower cholesterol levels compared to other ethnic groups. For any elevated lipid level, such as LDL cholesterol, South Asians have a 50% higher risk of heart attack or stroke than those from a Caucasian background. The American College of Cardiology’s risk estimator demonstrates how demographic-specific data can help estimate cardiovascular risk more accurately. Yet, clinicians often lack guidelines to adjust lab parameters to account for such ethnic-specific risks.
Some other notable examples of health inequities stemming from race-based lab result interpretations include:
Kidney Function (eGFR) Adjustments
The estimated glomerular filtration rate (eGFR), a measure of kidney function, has historically included an adjustment factor for Black patients. This adjustment suggested that Black patients had higher kidney function than non-Black patients with the same lab values, potentially delaying eligibility for critical treatments like dialysis or kidney transplants. The prevailing consensus among experts is to eliminate this race-based adjustment, as it can obscure the actual health needs of Black patients. Instead, a uniform eGFR value should be applied to all patients for a more equitable approach.
Heart Failure Risk Scores
Heart failure risk scores are sometimes calculated using algorithms that factor in a patient’s race. In certain cases, these algorithms assign a lower risk to Black patients compared to White patients with identical lab values and clinical symptoms, which can result in fewer referrals for advanced treatments. This underestimation of risk can delay necessary interventions for Black patients, leading to a potential gap in the quality of care.
Liver Function Test Adjustments
Some liver function tests also include race-based adjustments, which can lead to delayed diagnoses or treatments for Black patients. By assessing liver function differently based on racial categories rather than individual health data, these tests can hinder the early detection and management of liver diseases in minority populations.
Pulse Oximetry Inaccuracy
Pulse oximeters, devices used to measure blood oxygen levels, have given higher readings for Black patients than their actual oxygen saturation levels. This discrepancy can result in the underdiagnosis or inadequate treatment of respiratory conditions, as dangerously low oxygen levels may go undetected. This highlights the need for more accurate and equitable diagnostic tools for all patients.
Race-Based Lung Cancer Screening Criteria
Algorithms used in lung cancer screening eligibility often include race as a determining factor. For Black patients, who may already have a higher risk for lung cancer, this can mean a lower likelihood of meeting screening criteria due to race-based adjustments. As a result, Black patients might face delays in diagnosis and treatment, impacting their outcomes in the fight against lung cancer.
Precision Medicine and AI: The Way Forward
According to the CDC, approximately 70% of diagnoses rely on lab results. To achieve health equity, lab result interpretations should be adjusted based on an individual’s demographic profile based on the peer-reviewed academic medical research globally and validated against domestic populations of similar races and ethnicities. By doing so, we can help impact healthcare from a national population level to a local patient level.
Adjusting lab results to reflect diverse populations’ risks could enhance precision medicine and improve patient outcomes. Moreover, these adjustments are crucial as current medical practices and health systems, with their embedded biases, are often used as training datasets for artificial intelligence, potentially perpetuating racial disparities in future healthcare improvements.
By recalibrating our approach to health assessments and algorithms, we can improve healthcare on a national and local scale. A race-aware, rather than race-based, approach holds the promise of delivering equitable care and protecting both present and future generations.
Precision Medicine with Advanced Health Academy
Advanced Health Academy (AHA) provides precise and comprehensive interpretations of the most common labs, such as blood labs, which includes a CBC, CMP, lipid panel, thyroid panel, iron panel, and more. AHA automatically incorporates each patient’s demographics, including race and ethnicity, into lab interpretations to deliver precision medicine at the point of care.
As a result, AHA:
1. Sheds light on the complexity of the patient’s health and its root causes to reduce clinician cognitive load while upskilling their capabilities.
2. Discovers emerging chronic health issues and comorbidities earlier,
3. Presents corresponding ICD-10 codes with 100% clinical documentation integrity, streamlining appropriate coding and billing while optimizing reimbursements.
To learn more, reach out to AHA today.
Further Reading and Resources
For more information on these topics, explore the following sources:
- American College of Cardiology Risk Estimator
- The Impact of Health Care Algorithms on Racial and Ethnic Disparities
- Health Affairs on Race-Aware Algorithms
- Promoting Equity In Clinical Decision Making: Dismantling Race-Based Medicine
- A closer look at the role of health care algorithms in racial and ethnic disparities
- Strengthening Clinical Laboratories
- US census data