Triglycerides: Diagnostic Significance and Clinical Insights
Authors: Payal Bhandari M.D, Tejal, Madison Granados
Contributors: Vivi Chador, Hailey Chin, Nigella Umali Ruguian, Amer Džanković
Key Insights
A triglyceride (TG) test helps assess the risk of metabolic disorders, atherosclerosis, and other chronic diseases. TG consists of one fat molecule and three glucose molecules, playing a key role in energy and metabolism. It comes from diet and follows two pathways: exogenous (digestive tract to liver) and endogenous (transport to tissues). Being water-insoluble, TG travels via lipoproteins—VLDL, LDL, and HDL—where higher protein density means lower fat content. Hyperlipidemia, marked by high TG-rich LDL and VLDL, can lead to organ damage, inflammation, hormonal imbalance, infections, and cancer. Managing TG levels through hydration, a plant-based diet, exercise, stress control, and, if needed, medication or surgery is essential for health.
What are Triglycerides?
Fat refers to triglycerides, composed of a glycerol backbone and three fatty acids (FA). Saturated fats have no double bonds, making them solid at room temperature, while unsaturated fats have double bonds, creating a bent structure and remaining liquid. Cholesterol and lipids include mono- and diglycerides, phospholipids, sterols, and free fatty acids (FFA), made of carbon, hydrogen, and oxygen. A total cholesterol test measures LDL, HDL, IDL, VLDL, and triglycerides.
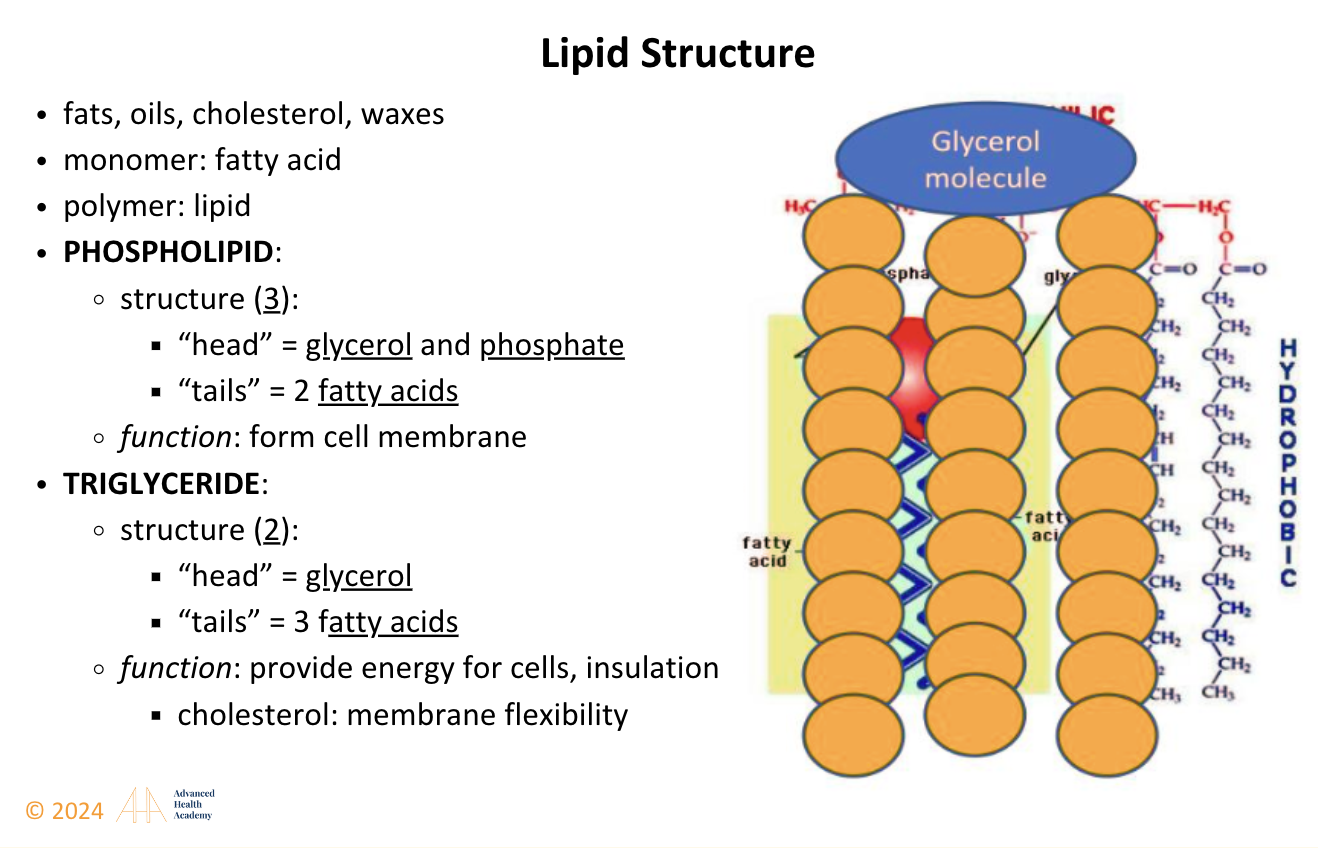
Figure 1: Lipid (Cholesterol) structure is present in all cellular membranes and lipoproteins.
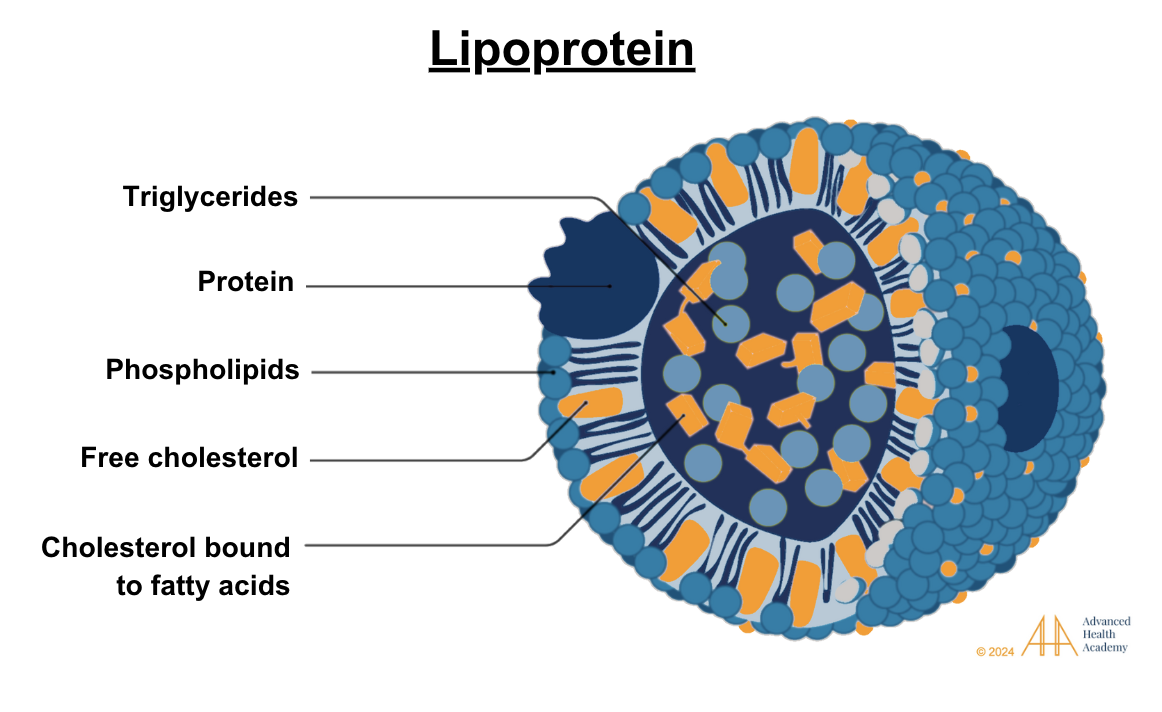
Figure 2: Lipoproteins have a core of cholesterol esters and triglycerides, surrounded by free cholesterol, phospholipids, and apoproteins, aiding their formation and function1.
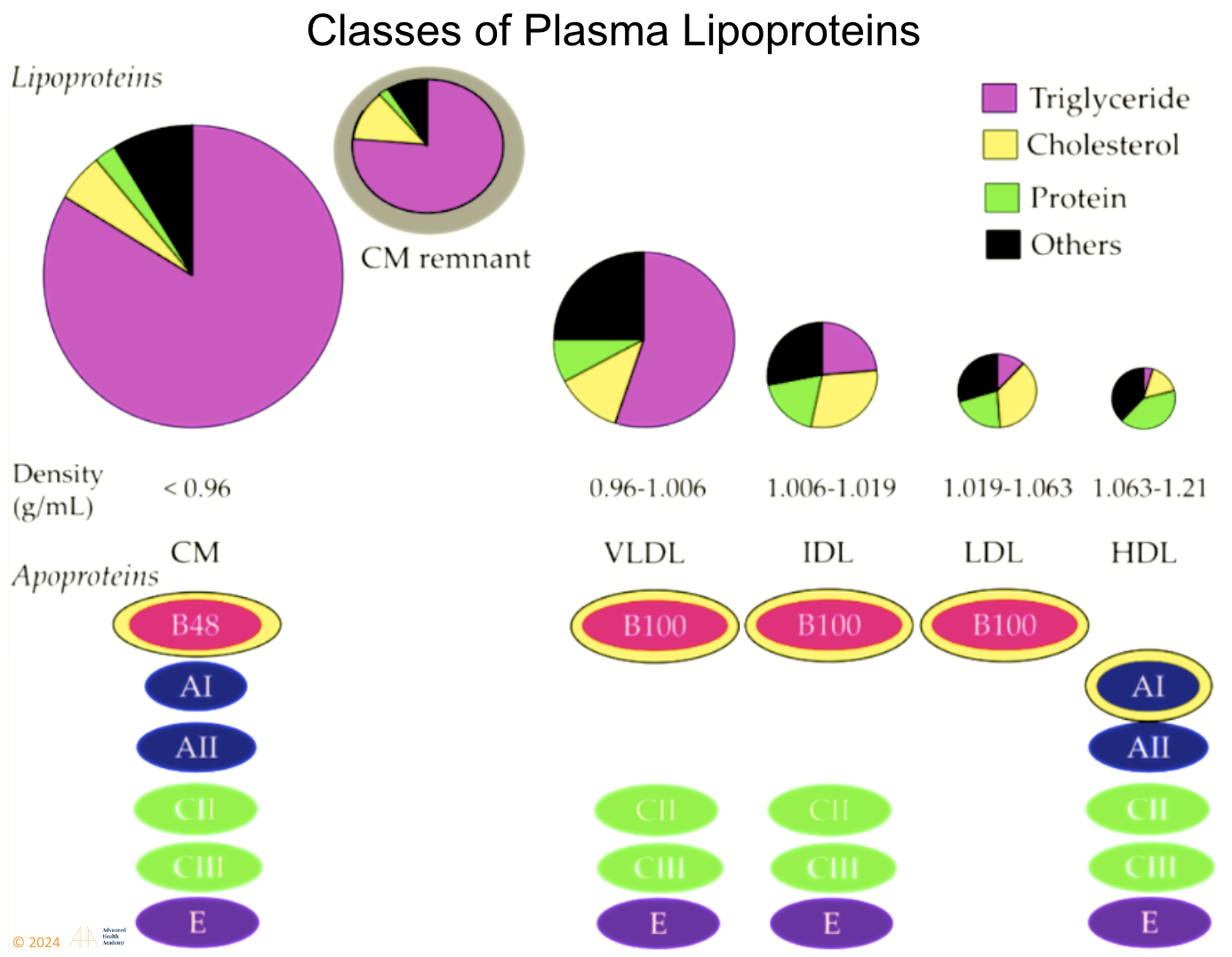
Figure 3: Plasma lipoproteins include chylomicrons, VLDL, IDL, LDL, HDL, and Lp(a). LDL, VLDL, and IDL promote atherosclerosis, while HDL protects against it. Since cholesterol and triglycerides are water-insoluble, they bind to apoproteins for transport and metabolism regulation.
Role of Triglycerides in the Body
Triglycerides (TG) help generate energy (ATP) through ketogenesis, producing ketones as an alternative fuel when glucose is low. Both ketones and glucose are vital for ATP production, sustaining life. Foods like fruits, vegetables, grains, and dairy break down into glucose, which enters the bloodstream and fuels cellular respiration. Figure 4 shows how glucose is transported to tissues that require immediate energy and undergo cellular respiration.
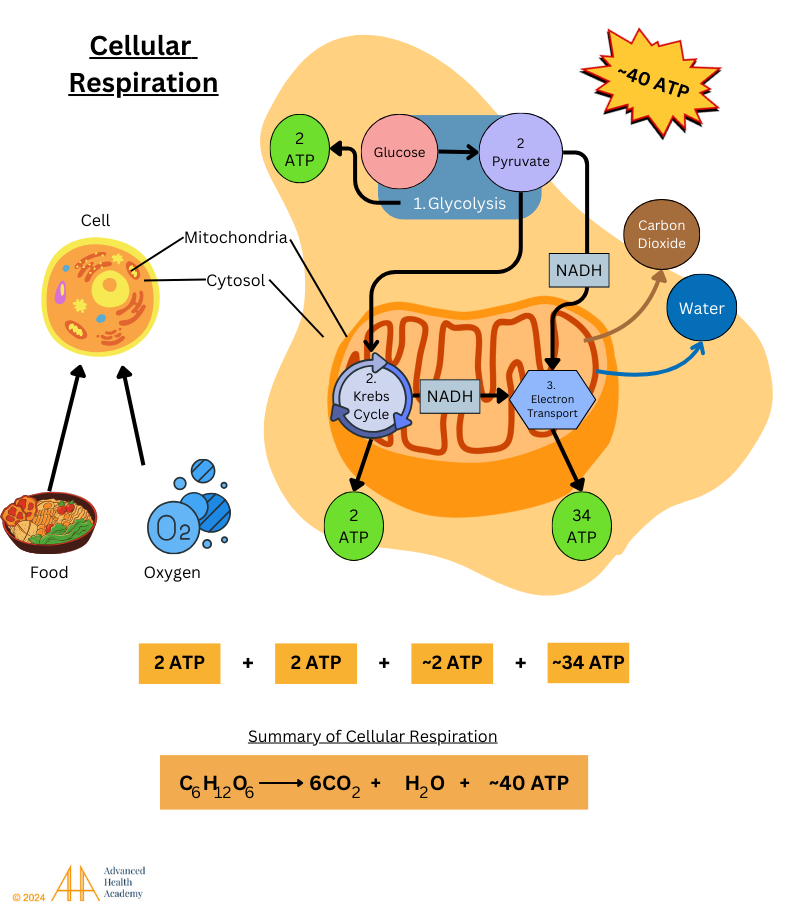
Figure 4: Cellular respiration converts food into energy (ATP, NADH, FADH) and releases CO₂ through exhalation. This three-step process produces most ATP in the mitochondria via the electron transport chain (34 ATP), plus 2 ATP from glycolysis and the Krebs cycle.
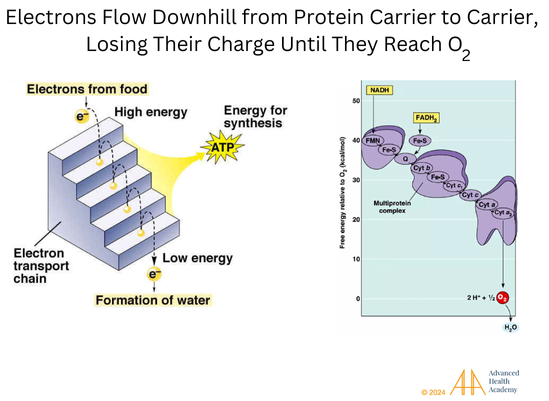
Figure 5: Electrons from chlorophyll-rich foods move through membrane proteins, losing charge until oxygen enables ATP production. Without oxygen (hypoxia), the electron transport chain stops, preventing ATP production, leading to cell death.
Excess glucose is stored as glycogen for ATP production during fasting, intense exercise, or high glucagon levels (as in diabetes). Ketogenesis supplies energy when the brain’s demand exceeds the body’s. Since the brain can’t use fatty acids directly, triglyceride glycerol converts to glucose via gluconeogenesis for ATP production.
Regulation of Triglycerides Synthesis
ATP is mainly produced from glucose through glycolysis. When sugar is low, gluconeogenesis in the liver, kidneys, and small intestine creates glucose for energy. In low-energy states or high glucagon levels (as in diabetes), ketogenesis uses triglycerides and proteins for fuel, especially in the brain, heart, and muscles. Since the brain can’t use fatty acids directly, triglyceride glycerol converts to glucose via gluconeogenesis for ATP production.
The body produces most triglycerides (TG), with a small portion from diet. Common TG-rich foods include dairy, red meat, eggs, poultry, fish, shellfish, oils, and some nuts. TG synthesis requires significant energy, involving enzymatic reactions across organs and cells .
Harvesting Energy (ATP) After A Meal
Food digestion in the small intestine releases glucose, fatty acids (FA), and amino acids (AA) into the blood, triggering insulin release to transport glucose for energy. Excess nutrients go to the liver, where glucose converts to glycogen, then FA or AA. FAs become triacylglycerol (TAG), stored or released as VLDL. Proteins and AAs provide energy or form new molecules. The liver detoxifies waste like reactive oxygen species (ROS), excreting it via stool, urine, and sweat.
Harvesting Energy During Short-Term Fasting
Gluconeogenesis synthesizes glucose from amino acids, lactate, and glycerol, depleting oxaloacetate and reducing ATP production. During fasting or intense exercise, glucagon and catecholamines increase, insulin decreases, and lipoprotein lipase (LPL) breaks down glycogen and triglycerides. Acetyl-CoA is beta-oxidized into ketones, mainly in the liver, via HMG CoA synthase. Acetoacetate converts to beta-hydroxybutyrate for ATP production, while some degrades into acetone and is exhaled .
Harvesting Energy During Prolonged Fasting
During fasting or intense exercise, the body runs low on energy and responds by:
The liver releasing stored fat (VLDL cholesterol).
Fat tissue breaking down fat (NEFAs, glycerol) to make ketones for energy.
Muscles breaking down protein (creatine), releasing lactate and alanine, which the liver uses to make glucose.
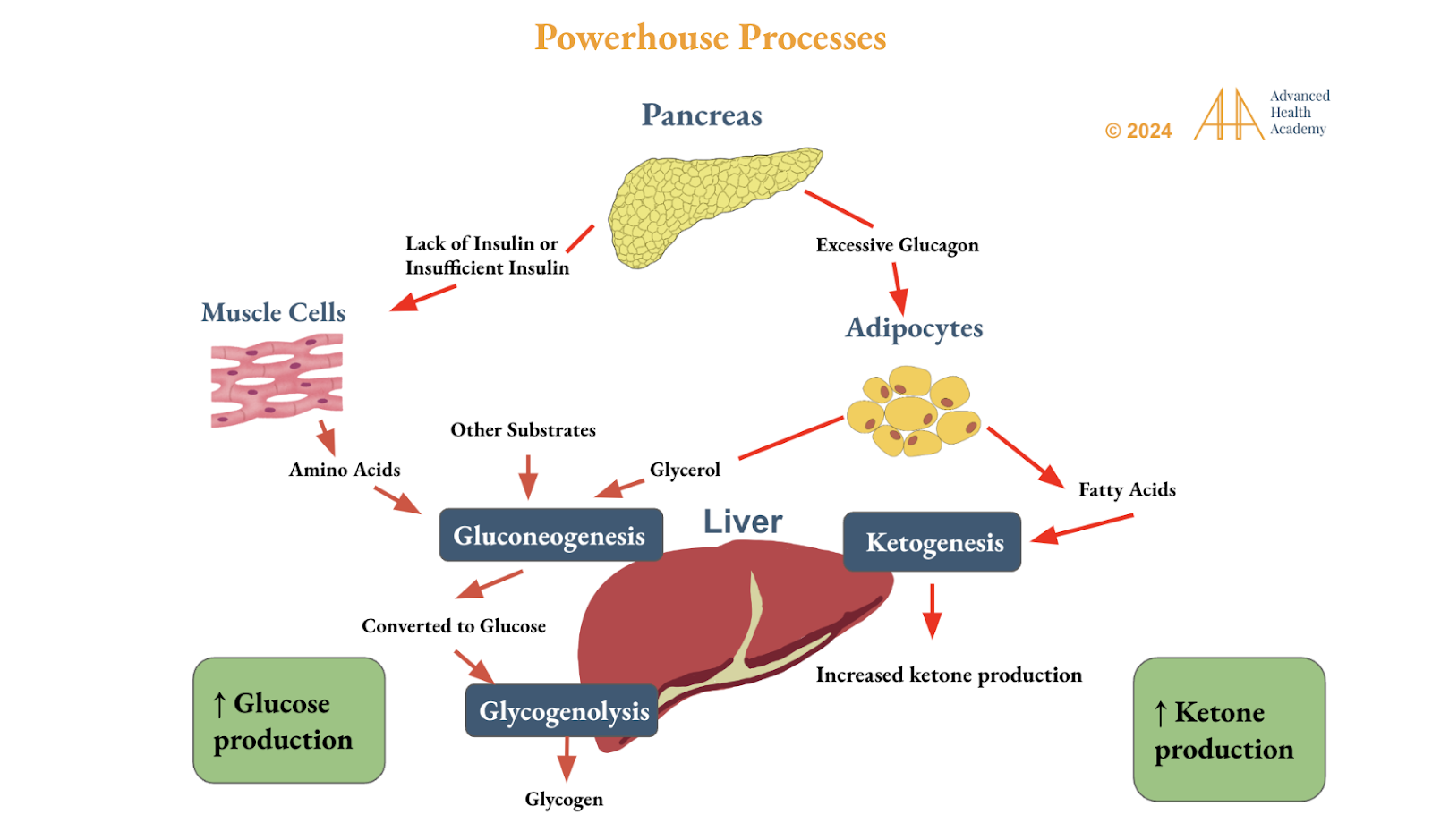
Figure 6: Circadian rhythm genes control how the liver produces glucose and ketones, helping the body get energy from fat, protein, and other sources. More ketone production keeps blood sugar stable, improves insulin and leptin sensitivity, and helps the brain rely less on carbs and protein. As a result, hunger, anxiety, stress hormones, and inflammation decrease.
Regulation of Triglyceride Metabolism
Glucagon, a hormone, helps break down triglyceride into free fatty acids (FFA) for energy or storage with the help of enzyme lipoprotein lipase (LPL). This happens in two ways:
Exogenous Pathway: The small intestine packs dietary fat into chylomicrons, mixing it with bile, cholesterol, and vitamins (A, D, E, K). These quickly move to the liver. A healthy liver can process up to 100g of fat daily without raising TG levels too much.
Endogenous Pathway: The liver processes TG in very-low-density lipoproteins (VLDL). As VLDL loses fat, it turns into LDL (“bad cholesterol”). More fat means larger VLDL and higher LDL levels.
Most FFAs come from food, while most cholesterol comes from bile (800–1200 mg vs. 200–500 mg from diet). A high-fat diet leads to larger chylomicrons, increasing LDL. During fasting, the liver makes fewer chylomicrons and VLDL, relying on stored fat.
After eating, 44% of VLDL’s TG comes from plasma FFA, 10% from diet, 15% from chylomicron remnants, and 8% from new cholesterol. During fasting, 77% comes from plasma FFA, with only 4% from new cholesterol.
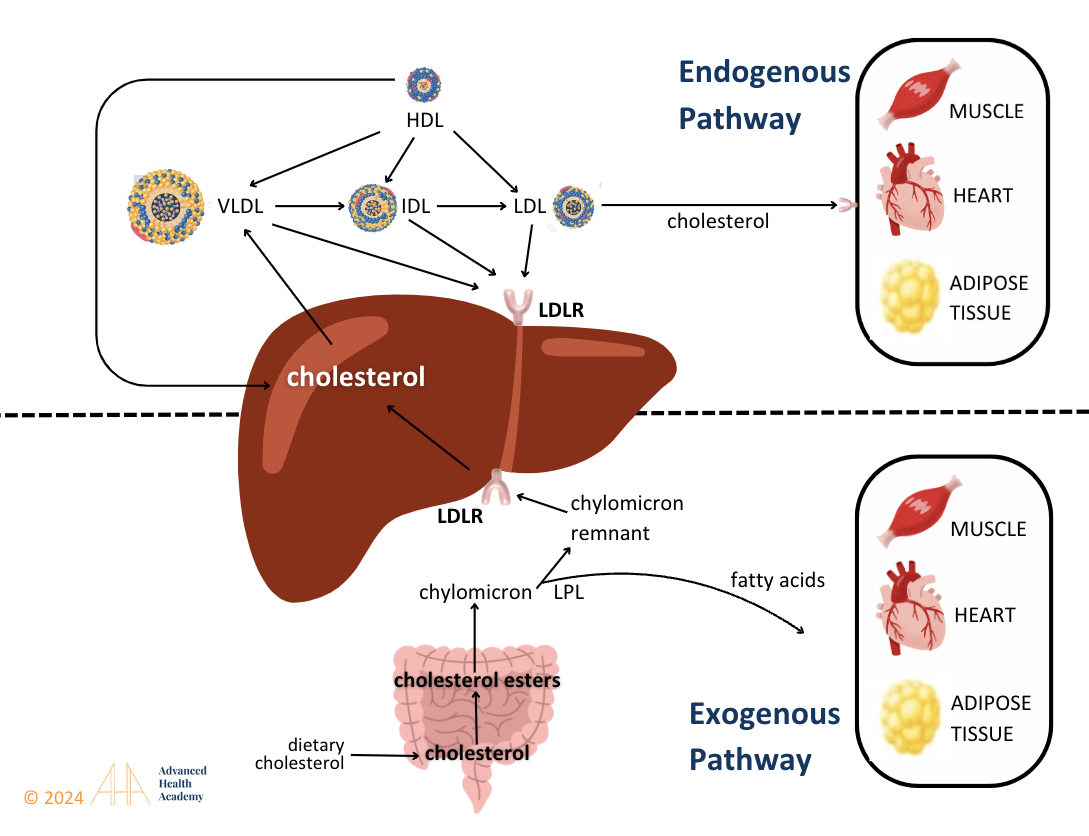
Figure 7: The body processes fat in two ways: exogenous (from food) and endogenous (made in the body). In the exogenous pathway, triglycerides (TG) from food turn into chylomicrons (CM) with help from an enzyme called LPL. CM carries fat through the lymph and blood, delivering it to muscles, organs, and fat tissue. LPL helps use TG for energy or store it as fat, shrinking CM. Some surface parts transfer to HDL, slowing TG breakdown. The leftover cholesterol in CM picks up apoE, forming CM remnants. In the endogenous pathway, the liver removes CM remnants from the blood and uses them to make VLDL cholesterol and bile acids.
Clinical Significance of Monitoring Abnormal Triglyceride Blood Levels5
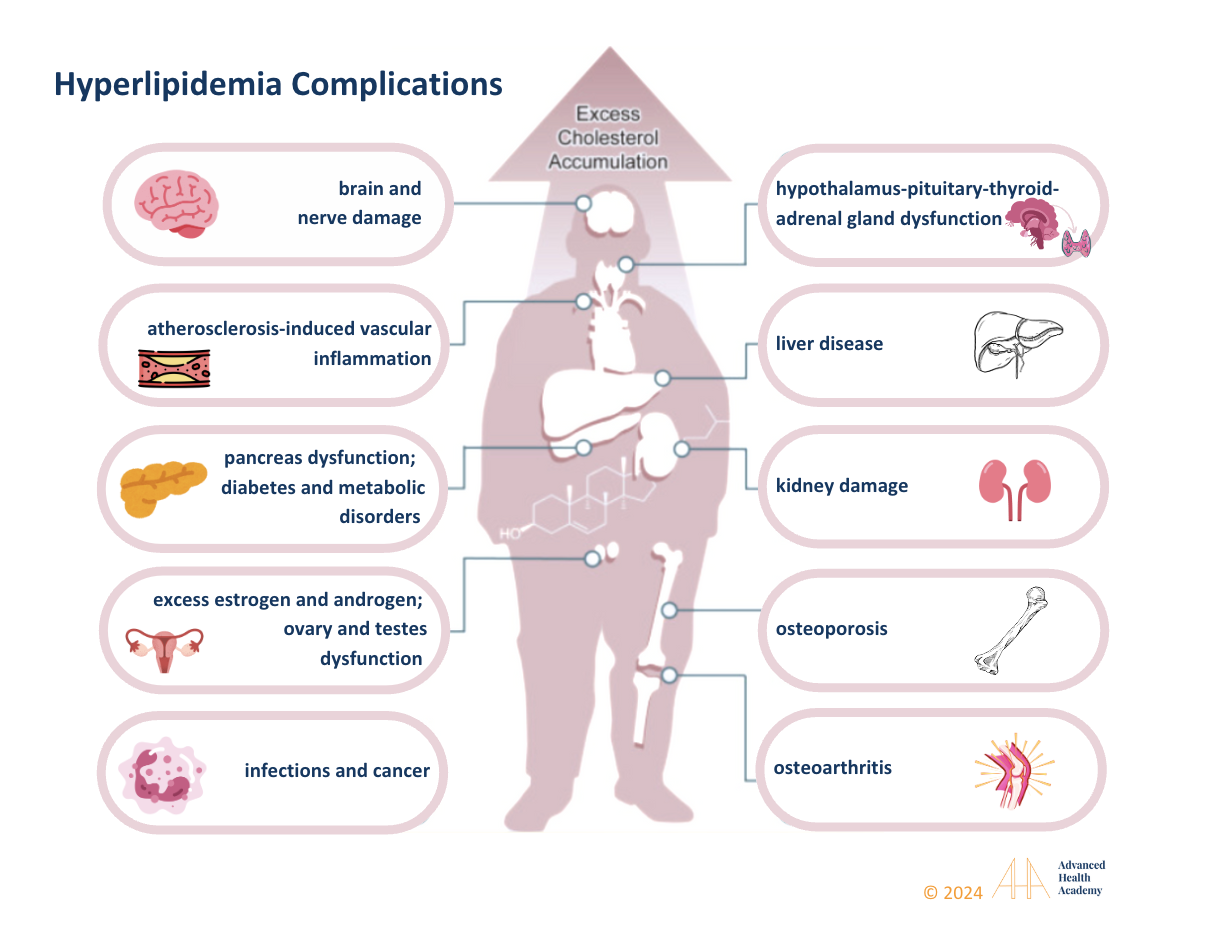
Figure 8: The clinical manifestations of extremely high triglyceride levels include, but are not limited to, multi-organ damage (such as the brain, liver, kidneys, bones, joints, digestive tract, and glands) which can lead to hormonal imbalances, infections, cancers, brittle bones (osteoporosis), osteoarthritis, diabetes, vascular diseases, and many more health conditions.
Hyperlipidemia means having too much fat (like triglycerides and cholesterol) in the blood. This can be inherited but is usually caused by unhealthy habits, such as eating too many calories and not burning enough fat for energy.
High triglyceride (TG) levels often come with high total cholesterol, VLDL, and LDL (bad cholesterol), and low HDL (good cholesterol). On the other hand, low TG levels are usually not a problem, especially if LDL and VLDL are also low and HDL is normal or high. Balanced TG levels support hormone production in the ovaries, testes, thyroid, and adrenal glands.
The main cause of abnormal triglyceride levels is poor gut health and reduced blood flow to organs. The gut helps digest food, absorb nutrients, and remove waste. When food stays too long in the stomach, it reduces healthy gut bacteria (dysbiosis) and can lead to nutrient deficiencies .
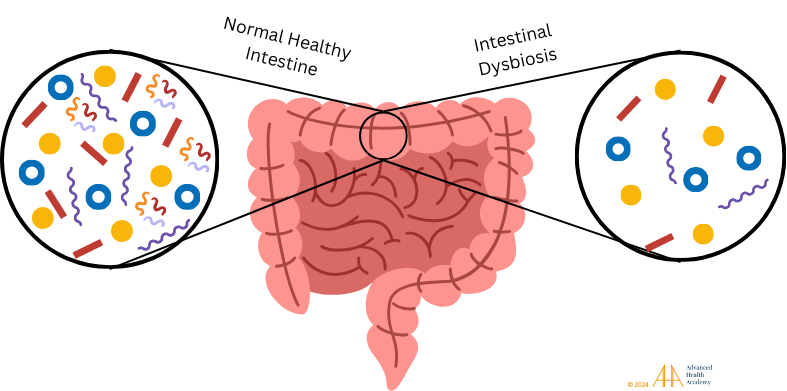
Figure 9: A healthy gut helps with digestion, nutrient absorption, and waste removal. Dysbiosis, or an imbalance of gut bacteria, can harm metabolism and increase inflammation and harmful microbes.
Dysbiosis (gut bacteria imbalance) disrupts how the body processes proteins, fats, and sugars and affects the production of key proteins and vitamins. This leads to undigested food particles and waste entering the bloodstream, thickening the blood and reducing oxygen to tissues. The liver turns excess food into fat, which gets stored in organs and fat cells.
Chronic dysbiosis and poor blood flow reduce energy production and cause inflammation that damages cells and genes. White blood cells focus on cleaning up damage and undigested food instead of fighting infections. This can lead to autoimmune issues, blood vessel damage, and artery problems. High blood triglycerides increase the risk of diseases, infections, cancer, and organ damage.
The consequences of high triglyceride (TG) blood levels include, but are not limited to the following diseases:
Atherosclerosis-Induced Vascular Inflammation
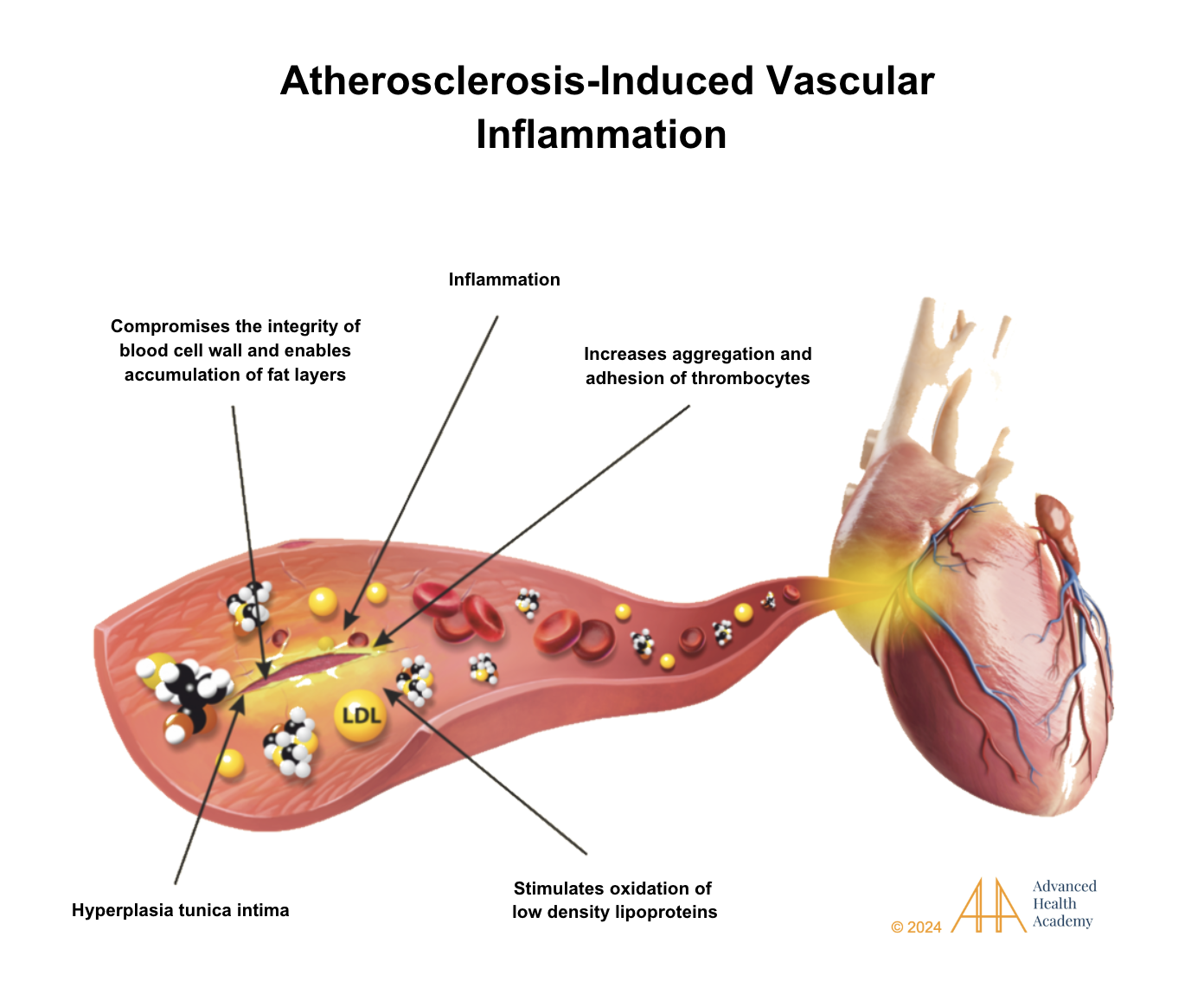
Figure 11: Atherosclerosis causes blood vessels to thicken with plaque, blocking blood flow. This happens when LDL cholesterol oxidizes and platelets form clots. Fat buildup inside the vessels raises blood pressure and redirects blood, causing it to back up into organs like the heart, liver, and legs, making them enlarge and work less efficiently.
Atherosclerosis causes inflammation in blood vessels and fat buildup in organs, which harms their function. For example, too much cholesterol in the pancreas damages cells and lowers hormone production, like insulin. This makes it harder to use glucose and increases blood sugar and reactive oxygen species (ROS) levels. The liver then makes more glucose, stops burning fat for energy, and raises levels of fats and proteins in the blood. This thickens the blood, reduces oxygen flow, and leads to cell damage and changes in metabolism.
Dysregulated Hormonal and Energy Balance
Elevated triglyceride (TG) levels are linked to long-term stress, which activates the body’s “fight-or-flight” response. This process involves the hypothalamus, pituitary gland, and adrenal glands, which release stress hormones like cortisol. These hormones then trigger the release of thyroid hormones (T3 and T4) by the thyroid gland. T4 is mostly converted to the more active T3 in the body, which boosts energy production.
While hyperthyroidism and short-term thyroid hormone use can increase fat metabolism, long-term hormone therapy or thyroid problems disrupt the body’s ability to regulate hormones and energy. This leads to more fat storage and less fat burning. It also increases glucose production, raising blood sugar, insulin, and harmful molecules like reactive oxygen species (ROS). ROS reduces the body’s ability to process LDL cholesterol, leading to higher levels of triglycerides (TG), VLDL, and LDL cholesterol in the blood.
High TG levels can cause fat to build up around internal organs and lead to fat loss in areas with more energy-burning cells. This disrupts cholesterol metabolism and may contribute to fat build-up in arteries, raising the risk of atherosclerosis and vascular diseases. It can also cause autoimmune disorders like Hashimoto’s thyroiditis, Graves’ disease, Cushing’s syndrome, Addison’s disease, and diabetes. Symptoms of these conditions can include irregular periods, polycystic ovary syndrome (PCOS), infertility, bone issues, fatigue, skin problems, and more. For instance, low blood flow to bones can weaken bone density, making fractures and skin problems like eczema or psoriasis more likely.
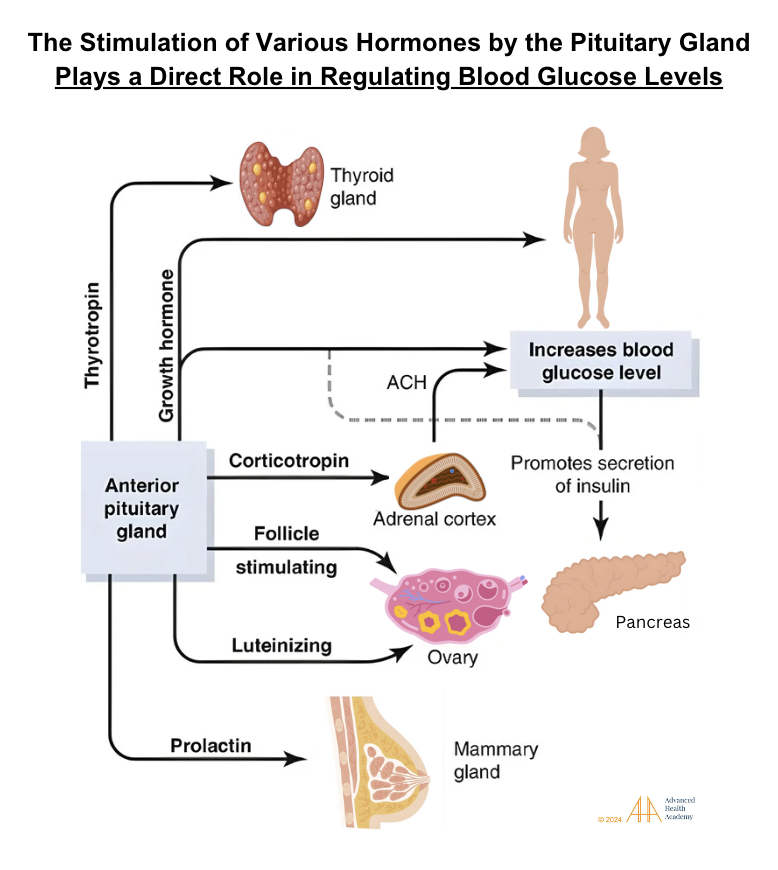
Figure 11: The pituitary gland makes hormones that help control energy balance and signal other glands. These include thyroid-stimulating hormone, corticotropin, growth hormone, and others. People with pituitary disorders often need lifelong treatment and support to manage issues like high blood sugar, triglycerides, and cholesterol.
A study in China found that people with subclinical hypothyroidism and higher cholesterol levels (>200 and >240 mg/dL) had a 6 to 15 times greater risk of developing overt hypothyroidism over three years. This link remained even after adjusting for factors like age, sex, BMI, diabetes, and high blood pressure. Statin drugs temporarily improved remission rates in subclinical hypothyroidism (50% vs. 15.4%) .
Many studies show that high-fat diets from animal products and, to a lesser extent, nuts can reduce the production of enzymes that help make testosterone. High levels of 25-hydroxycholesterol in the testicles can also lower testosterone production by affecting receptors. On the other hand, a plant-based diet, especially one rich in green vegetables, can lower harmful cholesterol levels and improve the processes that produce testosterone. Additionally, losing 5-10% of body weight can improve cholesterol, insulin sensitivity, and lower excess androgen production .
Autoimmune Disorders
Rheumatoid arthritis (RA), lupus (SLE), inflammatory bowel disease (IBD), ankylosing spondylitis, Sjögren’s syndrome, polymyalgia rheumatica, gum disease, multiple sclerosis, and HIV/AIDS are all linked to high triglyceride (fat) levels in the blood. These high levels are connected to inflammation in the blood vessels and autoimmune diseases . A study of 111,758 patients with 24 studies found that people with RA had a 50% higher risk of death compared to others. RA patients also face a similar risk of heart problems as people with diabetes. Autoimmune diseases often cause changes in lipid (fat) levels which involve 137:
Decrease in HDL-cholesterol and apolipoprotein A-I.
Elevated serum triglyceride and lipoprotein (a) levels.
Decreasing total and LDL cholesterol is associated with severe autoimmune cases.
Chronic Liver Dysfunction and Damage
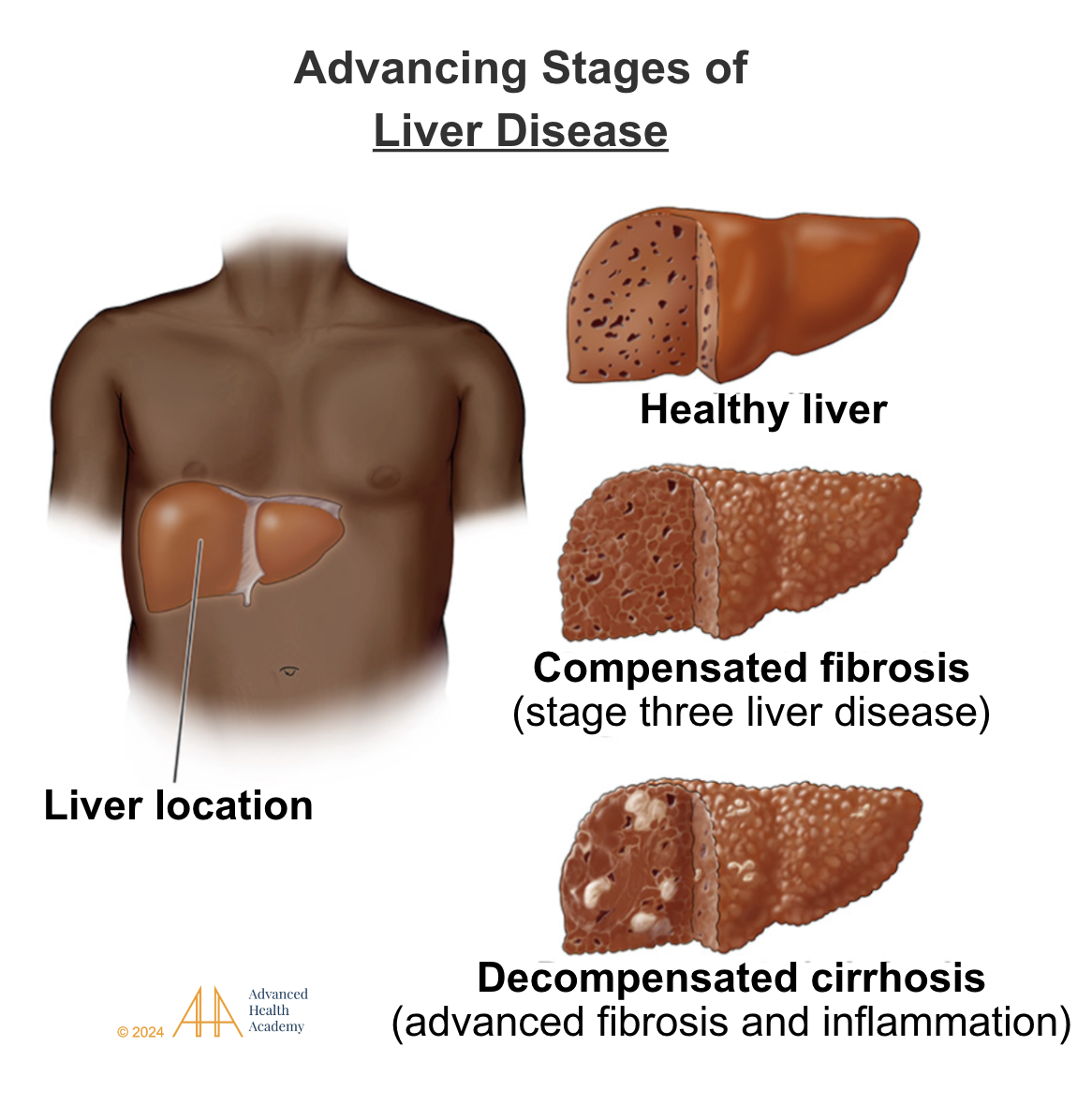
Figure 12: The liver is the central organ responsible for metabolizing fat (triglyceride), synthesizing new proteins (e.g., apoproteins) and amino acids, and detoxifying cellular waste. Liver dysfunction and damage are associated with excess proinflammatory cholesterol and proteins in the circulation shifting vital nutrients and oxygen away from various organs being able to harvest energy and sustain normal physiologic functions. Chronic inflammation is closely linked to high triglyceride levels and the direct harm liver cells suffer, resulting in conditions such as steatohepatitis, fibrosis, and cirrhosis.
Chronic Kidney Dysfunction and Damage
Many studies have shown that a high-fat diet can cause fat buildup in the kidneys, which harms cells and creates scar tissue that interferes with kidney function. A 2020 study in the Zhejiang population found that higher triglyceride (TG) levels in the blood were linked to faster kidney decline and a higher risk of chronic kidney disease (CKD). A review of 59 studies on cholesterol-lowering statins showed that lowering LDL cholesterol and triglycerides can slow down kidney decline. Since people with CKD are more vulnerable to harm from medications, a diet focused on plants and free of nuts and oils can help reduce kidney damage and complications from high cholesterol.
Skin Disorders
Excess fat on the skin can damage cells and cause the production of sebum, which changes the skin’s bacteria. This allows harmful bacteria like Propionibacterium to grow, leading to acne and other skin conditions linked to heart disease. People with acne often have lower good cholesterol, higher bad cholesterol, insulin problems, and hormone imbalances. Synthetic hormones like estrogen and testosterone can worsen skin and hair issues, causing excess hair growth, hair loss, and higher health risks.
The skin needs fat to produce hormones like DHT and estrogen. Too much DHT and cholesterol byproducts can slow hair growth and lead to hair loss 128.
Infections
Excess fat (triglycerides) in the blood makes it harder for cells to get energy and leads to the creation of harmful molecules that damage cells. This process causes inflammation, which helps viruses and bacteria attach to cholesterol in our cells, increasing the risk of infections . The severity of infections is closely linked to liver problems that affect fat processing and can predict higher death rates. Lipid imbalances often occur during infections and involves 137:
Decrease in HDL-cholesterol and apolipoprotein A-I.
Elevated serum triglyceride and lipoprotein (a) levels.
Decreasing total cholesterol and LDL-cholesterol is associated with severe infections.
Cancer Growth and Migration
Studies show that high levels of triglycerides, VLDL, and LDL cholesterol in the blood are linked to certain cancers. These fats increase the amount of oxidized cholesterol taken up by tumor cells, which helps them grow and spread. Blood levels of 25-hydroxycholesterol that are too high or too low are also tied to lower survival rates in cancer patients. The following cancers have a direct link to abnormal triglyceride levels: pancreatic , colon, breast (especially in overweight or obese people) , prostate , liver, lung , ovarian cancer, and chronic lymphocytic leukemia (CLL).
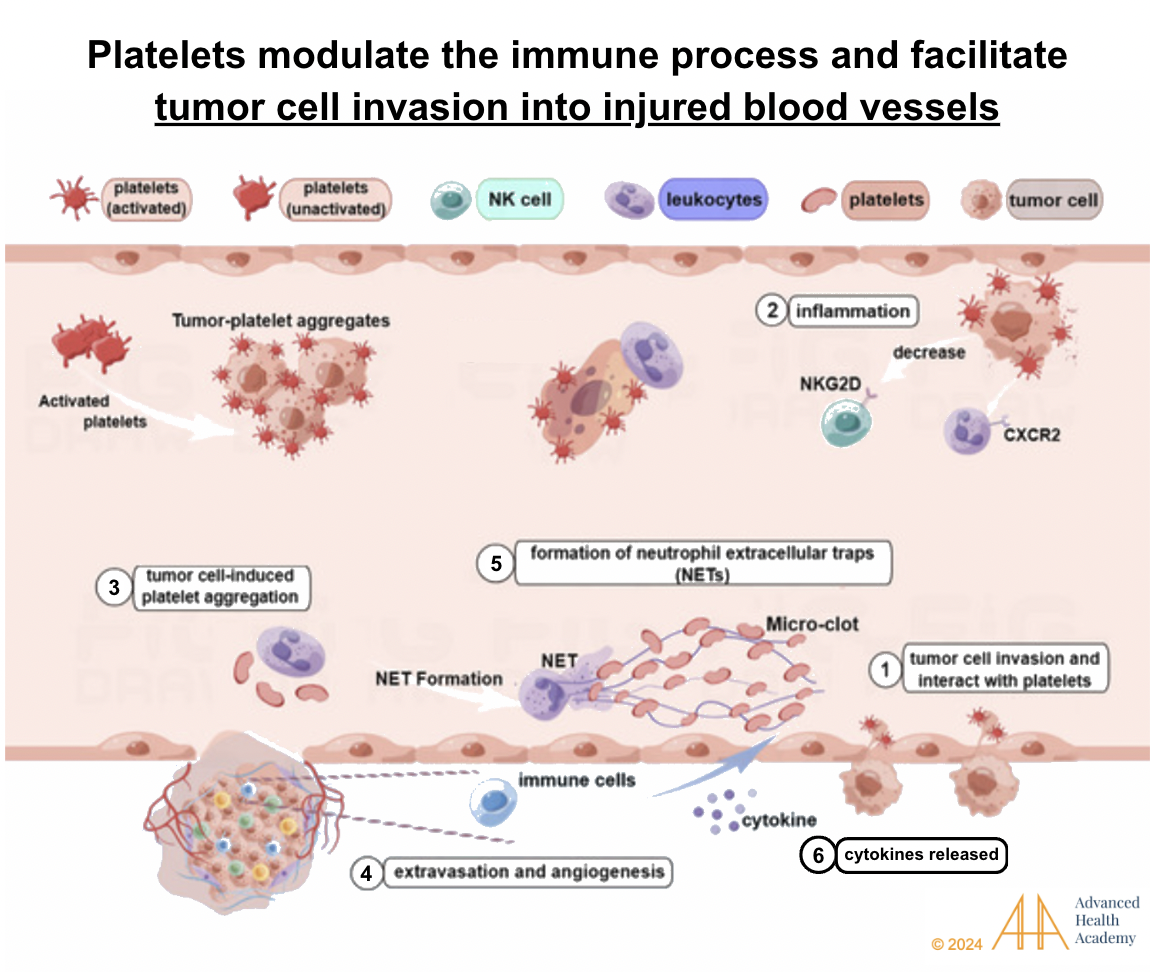
Figure 13: Oxidized cholesterol in the blood helps cancer grow and spread. Tumor cells attach to it and interact with platelets (1). Neutrophils protect tumor cells from being destroyed (2). Tumor cells cause platelets to form clots (3) and promote new blood vessels (4). Natural killer (NK) cells can’t destroy the tumor (5). Inflammation from these processes damages red blood cells, which feeds tumor growth and spread.
Brain and Nerve Damage
The brain has more cholesterol than other parts of the body. Since fat and protein molecules in the blood can’t pass through the blood-brain barrier, brain cells need to make their own cholesterol to get energy and stay balanced. When triglyceride (fat) metabolism slows down, it reduces energy and causes the production of harmful molecules (ROS) that can damage the blood-brain barrier and disrupt neuron function. White blood cells and platelets try to repair the damage but end up using energy that could go toward clearing harmful proteins like beta-amyloid. This causes brain cells to make more cholesterol, boosting mitochondrial activity and worsening neuroinflammatory and neurodegenerative diseases :
Learning disabilities
Cerebrovascular dysfunction
Mild cognitive impairment (familial hypercholesterolemia)
Cognitive impairment with impaired blood-brain barrier and neuroinflammation (such as dementia 169 )
Depression, anxiety, and other mental health disorders
Prevalence and Statistics of High Triglyceride Blood Levels (Hypertriglyceridemia)
Hypertriglyceridemia contributes to 2.6 million deaths (4.5% of total) and 29.7 million DALYs (2% globally). In 2008, 39% of adults had high triglycerides, with the highest rates in Europe (54%) and the Americas (48%), where diets are rich in animal protein51. Africa (22.6%) and Southeast Asia (29%) had lower rates due to plant-based diets. Triglyceride prevalence also increased with income, affecting 25% in low-income countries, one-third in middle-income, and over 50% in high-income nations.
Conclusion
Managing high triglycerides involves lifestyle changes like a plant-forward diet, exercise, fasting, stress management, avoiding tobacco and alcohol, and maintaining a healthy weight. Medications may help short-term until habits improve. Since lipid profiles alone don’t fully assess health risks, monitoring apoproteins and lipoprotein size provides better insight. Factors like family history, age, gender, and other health conditions also influence risk, requiring a comprehensive approach.
Source References and Supplemental Research:
Feingold KR, Anawalt B, Blackman MR, et al. Introduction to Lipids and Lipoproteins. MDText.com, Inc.; 2000. www.endotext.org
Chait A, Ginsberg HN, Vaisar T, Heinecke JW, Goldberg IJ, Bornfeldt KE. Remnants of the Triglyceride-Rich Lipoproteins, Diabetes, and Cardiovascular Disease. Diabetes 2020; 69:508-516 [PMC free article] [PubMed]
Krauss RM, King SM. Remnant lipoprotein particles and cardiovascular disease risk. Best Pract Res Clin Endocrinol Metab 2023; 37:101682 [PubMed]
Berneis KK, Krauss RM. Metabolic origins and clinical significance of LDL heterogeneity. J Lipid Res 2002; 43:1363-1379 [PubMed]
Asztalos BF, Niisuke K, Horvath KV. High-density lipoprotein: our elusive friend. Curr Opin Lipidol 2019; 30:314-319 [PubMed]
Thakkar H, Vincent V, Sen A, Singh A, Roy A. Changing Perspectives on HDL: From Simple Quantity Measurements to Functional Quality Assessment. J Lipids 2021; 2021:5585521 [PMC free article] [PubMed]
Thomas SR, Zhang Y, Rye KA. The pleiotropic effects of high-density lipoproteins and apolipoprotein A-I. Best Pract Res Clin Endocrinol Metab 2023; 37:101689 [PubMed]
Julve J, Martin-Campos JM, Escola-Gil JC, Blanco-Vaca F. Chylomicrons: Advances in biology, pathology, laboratory testing, and therapeutics. Clin Chim Acta 2016; 455:134-148 [PubMed]
Daoud E, Scheede-Bergdahl C, Bergdahl A. Effects of Dietary Macronutrients on Plasma Lipid Levels and the Consequence for Cardiovascular Disease. Journal of Cardiovascular Development and Disease. 2014; 1:201-213. 10.3390/jcdd1030201.
Gerber PA, Nikolic D, Rizzo M. Small, dense LDL: an update. Curr Opin Cardiol. 2017 Jul;32(4):454-459. doi: 10.1097/HCO.0000000000000410. PMID: 28426445.
Thomas A. B. Sanders (2016): “The Role of Fats in Human Diet.” Pages 1-20 of Functional Dietary Lipids. Woodhead/Elsevier, 332 pages. ISBN 978-1-78242-247-1doi:10.1016/B978-1-78242-247-1.00001-6
Entry for “fat” Archived 2020-07-25 at the Wayback Machine in the online Merriam-Webster dictionary, sense 3.2. Accessed on 2020-08-09
Wu, Yang; Zhang, Aijun; Hamilton, Dale J.; Deng, Tuo (2017). “Epicardial Fat in the Maintenance of Cardiovascular Health.” Methodist DeBakey Cardiovascular Journal. 13 (1): 20–24. doi:10.14797/mdcj-13-1-20. ISSN 1947-6094. PMC 5385790. PMID 28413578.
Feingold KR, Grunfeld C. Lipids: a key player in the battle between the host and microorganisms. J Lipid Res 2012; 53:2487-2489 [PMC free article] [PubMed]
White, Hayden; Venkatesh, Balasubramanian (2011). “Clinical review: Ketones and brain injury.” Critical Care. 15 (2): 219. doi:10.1186/cc10020. PMC 3219306. PMID 21489321
Abumrad NA, Davidson NO. Role of the gut in lipid homeostasis. Physiol Rev 2012; 92:1061-1085 [PMC free article] [PubMed]
Olivecrona G. Role of lipoprotein lipase in lipid metabolism. Curr Opin Lipidol 2016; 27:233-241 [PubMed]
Dallinga-Thie GM, Franssen R, Mooij HL, Visser ME, Hassing HC, Peelman F, Kastelein JJ, Peterfy M, Nieuwdorp M. The metabolism of triglyceride-rich lipoproteins revisited: new players, new insight. Atherosclerosis 2010; 211:1-8 [PMC free article] [PubMed]
M. Adiels, S.O. Olofsson, M.R. Taskinen, et al., Overproduction of very low-density lipoproteins is the hallmark of dyslipidemia in the metabolic syndrome, Arteriosclerosis, Thrombosis, Vasc. Biol. 28 (2008) 1225e1236.
Hooper AJ, Burnett JR, Watts GF. Contemporary aspects of the biology and therapeutic regulation of the microsomal triglyceride transfer protein. Circ Res 2015; 116:193-205 [PubMed] [Reference list]
S. Tiwari, S.A. Siddiqi, Intracellular trafficking and secretion of VLDL, Arteriosclerosis, Thrombosis, Vasc. Biol. 32 (2012) 1079e1086. DOI: 10.1161/ATVBAHA.111.241471
Daoud E, Scheede-Bergdahl C, Bergdahl A. Effects of Dietary Macronutrients on Plasma Lipid Levels and the Consequence for Cardiovascular Disease. Journal of Cardiovascular Development and Disease. 2014; 1:201-213. 10.3390/jcdd1030201.
Espenshade, P.J. SREBPs: sterol-regulated transcription factors. J. Cell Sci. 2006, 119, 973-976.
Dawidowicz, E.A. Dynamics of membrane lipid metabolism and turnover. Ann. Rev. Biochem. 1987, 56, 43–61.
Wang, H.H.; Garruti, G.; Liu, M.; Portincasa, P.; Wang, D.Q.-H. Cholesterol and Lipoprotein Metabolism and Atherosclerosis: Recent Advances in Reverse Cholesterol Transport. Ann. Hepatol. 2017, 16 (Suppl. S1), S27–S42.
Sacks, F.M.; Lichtenstein, A.H.; Wu, J.H.; Appel, L.J.; Creager, M.A.; Kris-Etherton, P.M.; Miller, M.; Rimm, E.B.; Rudel, L.L.; Robinson, J.G. and Stone, N.J. Dietary Fats and Cardiovascular Disease: A Presidential Advisory From the American Heart Association. Circulation 2017, 136, e1–e23.
Di Ciaula, A.; Garruti, G.; Baccetto, R.L.; Molina-Molina, E.; Bonfrate, L.; Portincasa, P.; Wang, D.Q.. Bile acid physiology. Ann. Hepatol. 2017, 16, s4–s14.
Cox, R.A.; García-Palmieri, M.R. Cholesterol, Triglycerides, and Associated Lipoproteins. In Clinical Methods: The History, Physical, and Laboratory Examinations; Walker, H.K., Hall, W.D., Hurst, J.W., Eds.; Butterworths: Boston, MA, USA, 2011.
Piskin E, Cianciosi D, Gulec S, Tomas M, Capanoglu E. Iron Absorption: Factors, Limitations, and Improvement Methods. ACS Omega. 2022 Jun 21; 7(24): 20441–20456. doi: 10.1021/acsomega.2c01833
Benkhedda K.; L’abbé M. R.; Cockell K. A. Effect of Calcium on Iron Absorption in Women with Marginal Iron Status. Br. J. Nutr. 2010, 103 (5), 742–748. 10.1017/S0007114509992418.
Ziegler E.E. Consumption of cow’s milk as a cause of iron deficiency in infants and toddlers. Nutr. Rev. 2011;69:37–42. doi: 10.1111/j.1753-4887.2011.00431.x.
Bondi S.A., Lieuw K. Excessive Cow’s Milk Consumption and Iron Deficiency in Toddlers, Two Unusual Presentations and Review. ICAN Infant Child Adolesc. Nutr. 2009;1:133–139. doi: 10.1177/1941406409335481. [CrossRef]
Gifford GE, Duckworth DH. Introduction to TNF and related lymphokines. Biotherapy. 1991;3:103–111
De Chiara, F., Checcllo, C. U., & Azcón, J. R. (2019). High protein diet and metabolic plasticity in Non-Alcoholic Fatty liver Disease: Myths and Truths. Nutrients, 11(12), 2985. https://doi.org/10.3390/nu11122985 [PubMed]
Esse, R.; Barroso, M.; Almeida, I.; Castro, R. The contribution of homocysteine metabolism disruption to endothelial dysfunction: State-of-the-art. Int. J. Mol. Sci. 2019, 20, 867. [Google Scholar] [CrossRef] [Green Version].
Kruman, I.I.; Culmsee, C.; Chan, S.L.; Kruman, Y.; Guo, Z.; Penix, L.; Mattson, M.P. Homocysteine elicits a DNA damage response in neurons that promotes apoptosis and hypersensitivity to excitotoxicity. J. Neurosci. 2000, 20, 6920–6926.
Guoyao Wu; Yun-Zhong Fang; Sheng Yang; Joanne R. Lupton; Nancy D. Turner (2004). “Glutathione Metabolism and its Implications for Health”. Journal of Nutrition. 134 (3): 489–492. doi:10.1093/jn/134.3.489. PMID 14988435 [PubMed]
Pompella A, Visvikis A, Paolicchi A, De Tata V, Casini AF (October 2003). “The changing faces of glutathione, a cellular protagonist”. Biochemical Pharmacology. 66 (8): 1499–1503. doi:10.1016/S0006-2952(03)00504-5. PMID 14555227
S. Tiwari, S.A. Siddiqi, Intracellular trafficking and secretion of VLDL, Arteriosclerosis, Thrombosis, Vasc. Biol. 32 (2012) 1079e1086. DOI: 10.1161/ATVBAHA.111.241471
Reichert CO, Levy D, Bydlowski SP. Paraoxonase Role in Human Neurodegenerative Diseases. Antioxidants (Basel). 2020 Dec 24;10(1):11. doi: 10.3390/antiox10010011. PMID: 33374313; PMCID: PMC7824310.
Sengupta, S.; Chen, H.; Togawa, T.; DiBello, P.M.; Majors, A.K.; Büdy, B.; Ketterer, M.E.; Jacobsen, D.W. Albumin thiolate anion is an intermediate in the formation of albumin-S-S-homocysteine. J. Biol Chem. 2001, 276, 30111–30117.
Diamond, J.R. Analogous Pathobiologic Mechanism in Glomerulosclerosis and Atherosclerosis. Kidney Int. 1991, 31, 29–34.
Chen, P.; Poddar, R.; Tipa, E.V.; Dibello, P.M.; Moraveca, C.D.; Robinson, K.; Green, R.; Kruger, W.D.; Garrow, T.A.; Jacobsen, D.W. Homocysteine Metabolism in Cardiovascular Cells and Tissues: Implication for Hyperhomocysteinemia and Cardiovascular Disease. Adv. Enzym. Regul. 1999, 39, 93–109.
Ho, P.I.; Ashline, D.; Dhitavat, S.; Ortiz, D.; Collins, S.C.; Shea, T.B.; Rogers, E. Folate deprivation induces neurodegeneration: Roles of oxidative stress and increased homocysteine. Neurobiol. Dis. 2003, 14, 32–42.
M.B. Fessler, The challenges and promise of targeting the Liver X Receptors for treatment of inflammatory disease, Pharmacol. Ther. (2017), https:// doi.org/10.1016/j.pharmthera.2017.07.010 pii: S0163-7258(17)30190-0.
S.D. Lee, P. Tontonoz, Liver X receptors at the intersection of lipid metabolism and atherogenesis, Atherosclerosis 242 (2015) 29e36.
D.S. Green, H.A. Young, J.C. Valencia, Current prospects of type II interferon gamma signaling and autoimmunity, J. Biol. Chem. 292 (2017) 13925e13933.
M. Buttet, H. Poirier, V. Traynard, et al., Deregulated lipid sensing by intestinal CD36 in diet-induced hyperinsulinemic obese mouse model, PLoS One 11 (2016), e0145626.
Main, P.A.; Angley, M.T.; O’Doherty, C.E.; Thomas, P.; Fenech, M. The potential role of the antioxidant and detoxification properties of glutathione in autism spectrum disorders: A systematic review and meta-analysis. Nutr. Metab. 2012, 9, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Desai, A.; Sequeira, J.M.; Quadros, E.V. The metabolic basis for developmental disorders due to defective folate transport. Biochimie 2016, 126, 31–42. [Google Scholar] [CrossRef]
Ali, A.; Waly, M.I.; Al-Farsi, Y.M.; Essa, M.M.; Al-Sharbati, M.M.; Deth, R.C. Hyperhomocysteinemia among Omani autistic children: A case-control study. Acta Biochim. Pol. 2011, 58, 547–551. [Google Scholar] [CrossRef]
Al-Farsi, Y.M.; Waly, M.I.; Deth, R.C.; Al-Sharbati, M.M.; Al-Shafaee, M.; Al-Farsi, O.; Al-Khaduri, M.M. Low folate and vitamin B12 nourishment is common in Omani children with newly diagnosed autism. Nutrition 2013, 29, 537–541. [Google Scholar] [CrossRef]
Fuentes-Albero, M.; Cauli, O. Homocysteine Levels in Autism Spectrum Disorder: A Clinical Update. Endocr. Metab. Immune Disord. Drug Targets 2018, 18, 289–296. [Google Scholar] [CrossRef]
Altun, H.; Kurutaş, E.B.; Şahin, N.; Güngör, O.; Findikli, E. The Levels of Vitamin D, Vitamin D Receptor, Homocysteine and Complex B Vitamin in Children with Autism Spectrum Disorders. Clin. Psychopharmacol. Neurosci. 2018, 16, 383–390. [Google Scholar] [CrossRef]
Kałużna-Czaplińska, J.; Żurawicz, E.; Michalska, M.; Rynkowski, J. A focus on homocysteine in autism. Acta Biochim. Pol. 2013, 60, 137–142. [Google Scholar] [CrossRef] [PubMed]
Mattson, M.P.; Shea, T.B. Folate and homocysteine metabolism in neural plasticity and neurodegenerative disorders. Trends Neurosci. 2003, 26, 137–146. [Google Scholar] [CrossRef]
Ho, P.I.; Ortiz, D.; Rogers, E.; Shea, T.B. Multiple aspects of homocysteine neurotoxicity: Glutamate excitotoxicity, kinase hyperactivation and DNA damage. J. Neurosci. Res. 2002, 70, 694–702. [Google Scholar] [CrossRef] [PubMed]
Fulceri, F.; Morelli, M.; Santocchi, E.; Cena, H.; Del Bianco, T.; Narzisi, A.; Calderoni, S.; Muratori, F. Gastrointestinal symptoms and behavioral problems in preschoolers with Autism Spectrum Disorder. Dig. Liver Dis. 2016, 48, 248–254. [Google Scholar] [CrossRef]
Chauhan, A.; Audhya, T.; Chauhan, V. Brain region-specific glutathione redox imbalance in autism. Neurochem. Res. 2012, 37, 1681–1689. [Google Scholar] [CrossRef]
Rossignol, D.A.; Frye, R.E. Evidence linking oxidative stress, mitochondrial dysfunction, and inflammation in the brain of individuals with autism. Front. Physiol. 2014, 5, 150. [Google Scholar] [CrossRef] [Green Version]
Frye, R.E.; Melnyk, S.; Fuchs, G.; Reid, T.; Jernigan, S.; Pavliv, O.; Hubanks, A.; Gaylor, D.W.; Walters, L.; James, S.J. Effectiveness of methylcobalamin and folinic acid treatment on adaptive behavior in children with autistic disorder is related to glutathione redox status. Autism Res. Treat. 2013, 2013, 609705. [Google Scholar] [CrossRef]
Sun, C.; Zou, M.; Zhao, D.; Xia, W.; Wu, L. Efficacy of Folic Acid Supplementation in Autistic Children Participating in Structured Teaching: An Open-Label Trial. Nutrients 2016, 8, 337. [Google Scholar] [CrossRef] [Green Version]
Bottiglieri, T. Folate, vitamin B12, and neuropsychiatric disorders. Nutr. Rev. 1996, 54, 382–390. [Google Scholar] [CrossRef] [PubMed]
Ezzaher, A.; Mouhamed, D.H.; Mechri, A.; Omezzine, A.; Neffati, F.; Douki, W.; Bouslama, A.; Gaha, L.; Najjar, M.F. Hyperhomocysteinemia in Tunisian bipolarI patients. Psychiatry Clin. Neurosci. 2011, 65, 664–671. [Google Scholar] [CrossRef]
Kim, H.; Lee, K.J. Serum homocysteine levels are correlated with behavioral and psychological symptoms of Alzheimer’s disease. Neuropsychiatr. Dis. Treat. 2014, 10, 1887–1896. [Google Scholar] [CrossRef] [Green Version]
Altun, H.; Şahin, N.; Belge Kurutaş, E.; Güngör, O. Homocysteine, Pyridoxine, Folate and Vitamin B12 Levels in Children with Attention Deficit Hyperactivity Disorder. Psychiatr. Danub. 2018, 30, 310–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Brunzell J, Rohlfing J. The Effects of Diuretics and Adrenergic-Blocking Agents on Plasma Lipids. West J Med. 1986 Aug; 145(2): 210–218. PMC1306877
Wolinsky H. The effects of beta-adrenergic blocking agents on blood lipid levels. Clin Cardiol. 1987 Oct;10(10):561-6. Doi: 10.1002/clc.4960101010
Stocker R, Yamamoto Y, McDonagh AF, Glazer AN, Ames BN. Bilirubin is an antioxidant of possible physiological importance. Science. 1987;235(4792):1043-6.
Baranano DE, Rao M, Ferris CD, Snyder SH. Biliverdin reductase: a major physiologic cytoprotectant. Proc Natl Acad Sci USA. 2002;99(25):16093-8.
B.R. Barrows, E.J. Parks, Contributions of different fatty acid sources to very low-density lipoprotein-triacylglycerol in the fasted and fed states, J. Clin. Endocrinol. Metabolism 91 (2006) 1446e1452. DOI: 10.1210/jc.2005-1709