Phosphorus: Diagnostic Significance and Clinical Insights
Authors: Dr. Payal Bhandari, M.D., Hailey Chin
Contributors: Vivi Chador

Key Insights
Phosphorus is important for energy production, bone health, and cell function. It helps form DNA, RNA, and ATP, which transfers energy in the body. Blood phosphorus levels are tested to check for imbalances, which can cause bone pain, muscle weakness, fatigue, and brain issues. Testing is important for monitoring chronic conditions like kidney disease, diabetes, and hormonal problems. Regular tests can help detect and manage these conditions early, allowing for dietary and lifestyle changes to prevent serious health issues.
What is Phosphorus?
Phosphorus is a key mineral for many body functions, such as energy metabolism, bone health, and kidney function. It’s mainly found as phosphate, which is part of ATP, the energy used by cells. ATP is made through cellular respiration, where phosphate is added to ADP to store and transfer energy. This energy is important for muscle contraction, protein building, and making DNA and RNA.
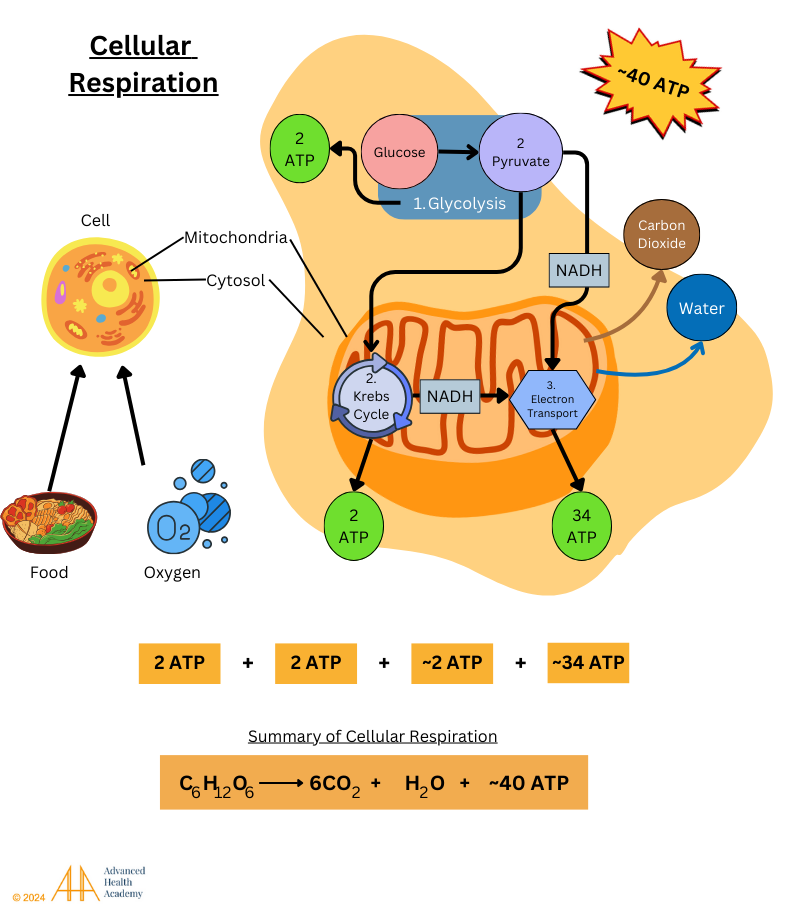
Figure 1: Cellular respiration is a process that converts energy from plants into molecules like ATP, NADH, and FADH. These molecules carry energy, and CO2 is released when we exhale. The process happens in three steps, with the most energy being produced in the electron transport chain in the mitochondria (34 ATP from this step, plus 2 ATP from glycolysis and the Krebs cycle).
Most phosphorus in the body is stored in bones and teeth, where it works with calcium to strengthen bones. A good balance of phosphorus and calcium helps prevent bone problems like osteoporosis, rickets, and osteomalacia. Phosphorus is also important for building cell membranes and supporting cell communication. Healthy phosphorus levels are crucial for many body functions and help prevent issues like heart disease and bone or kidney problems.

Figure 2: Phosphorus is important for energy production, bone health, and cell functions. It is a key part of ATP, which carries energy in cells. Phosphorus works with calcium to keep bones and teeth strong and helps control enzymes and receptors that regulate metabolism and cell communication. It also helps balance fluids and minerals like calcium, sodium, magnesium, and potassium. Keeping phosphorus levels steady is crucial for overall health.
Regulation of Phosphorus Levels in the Body
Phosphorus levels in the blood are controlled by hormones and organs like the kidneys and small intestine. The body adjusts how much phosphorus it absorbs, stores in bones, and excretes to keep blood levels balanced.
Phosphorus comes from foods like:
Seeds: Sunflower, chia, flaxseeds
Nuts: Almonds, cashews, walnuts
Legumes: Lentils, chickpeas, soy products
Whole grains: Quinoa, oats, brown rice
Vegetables: Potatoes, broccoli, Brussels sprouts
Nutritional yeast: High in phosphorus and B vitamins
After eating, phosphorus is absorbed in the small intestine and enters the bloodstream. It helps with fluid balance, energy, bone health, and cell function. Excess phosphorus is filtered by the kidneys and excreted in urine.
Two key hormones, parathyroid hormone (PTH) and fibroblast growth factor 23 (FGF-23), regulate phosphorus. PTH increases phosphorus excretion when calcium is low. FGF-23 helps control phosphorus levels by reducing reabsorption in the kidneys and activating vitamin D. High levels of PTH and FGF-23 can lead to imbalances in calcium, magnesium, vitamin D, and energy.
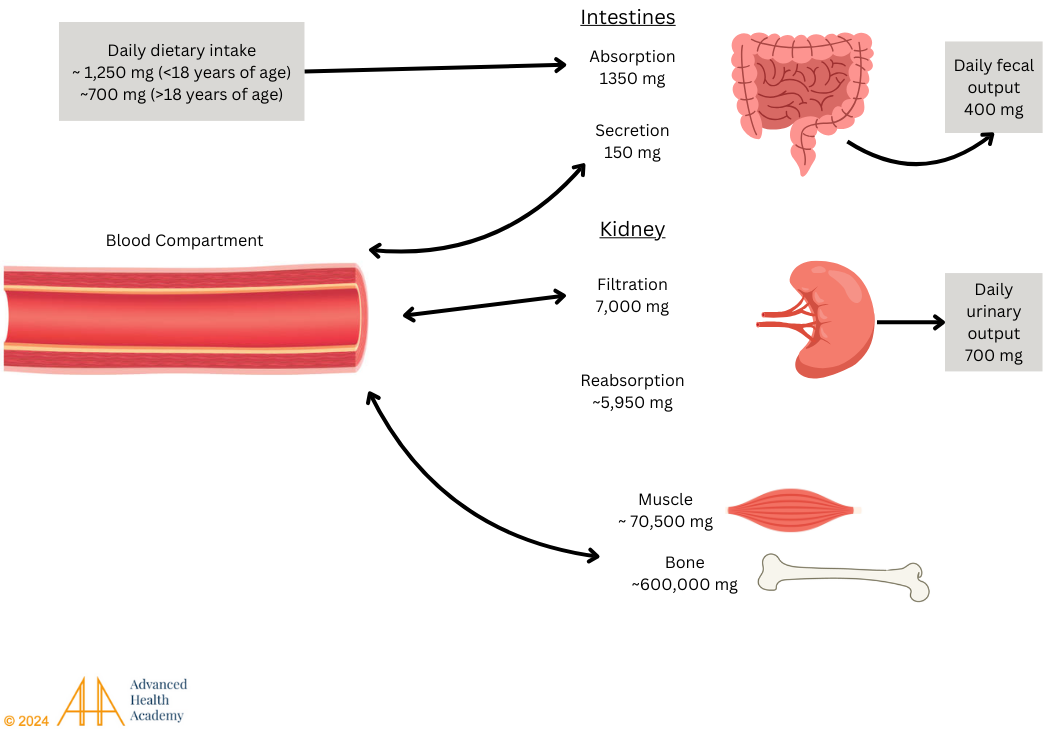
Figure 3: Phosphorus absorption primarily occurs in the small intestine. It is then released into the bloodstream, filtered by the kidneys, and reabsorbed. Most unused phosphorus is excreted in the urine, with a large percentage stored in the bones and skeletal muscles.
Clinical Significance of High Blood Phosphorus Levels
Secondary Hyperparathyroidism
High phosphorus levels in the blood (hyperphosphatemia) are common in people with kidney disease (CKD). When the kidneys can’t control phosphorus, it builds up in the blood and causes the parathyroid glands to release more parathyroid hormone (PTH), which weakens bones and increases the risk of fractures. High calcium levels can also harden blood vessels, affecting blood flow and organ health. Managing phosphorus is important in CKD to protect bones and reduce heart risks.
Dysbiosis and Atherosclerosis-Induced Cardiovascular Diseases
Blood plasma is mostly water (90%). High phosphate levels (hyperphosphatemia) can cause blood vessels to tighten, reducing blood flow and harming gut bacteria. This makes it harder to digest food, absorb nutrients, and remove waste. It also prevents the production of digestive enzymes and stomach acid (HCl). Without these, the body struggles to break down food and produce nitric oxide, which keeps arteries flexible and controls blood pressure. Low nitric oxide leads to undigested food and toxins in the body, damaging cells. This causes inflammation, blood clot formation, scarring, and new blood vessel growth, which is linked to atherosclerosis.
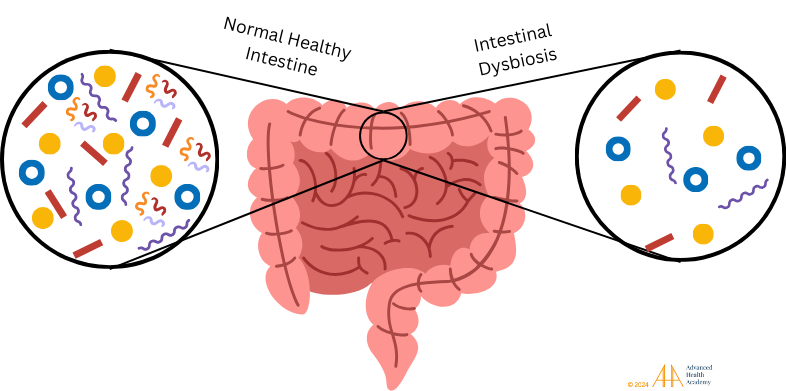
Figure 4: A healthy gut microbiota is important for digestion, nutrient absorption, and waste removal. Dysbiosis happens when healthy bacteria decrease, disrupting metabolism, reducing energy, and causing inflammation. This leads to more harmful pathogens and unhealthy cholesterol in the blood.
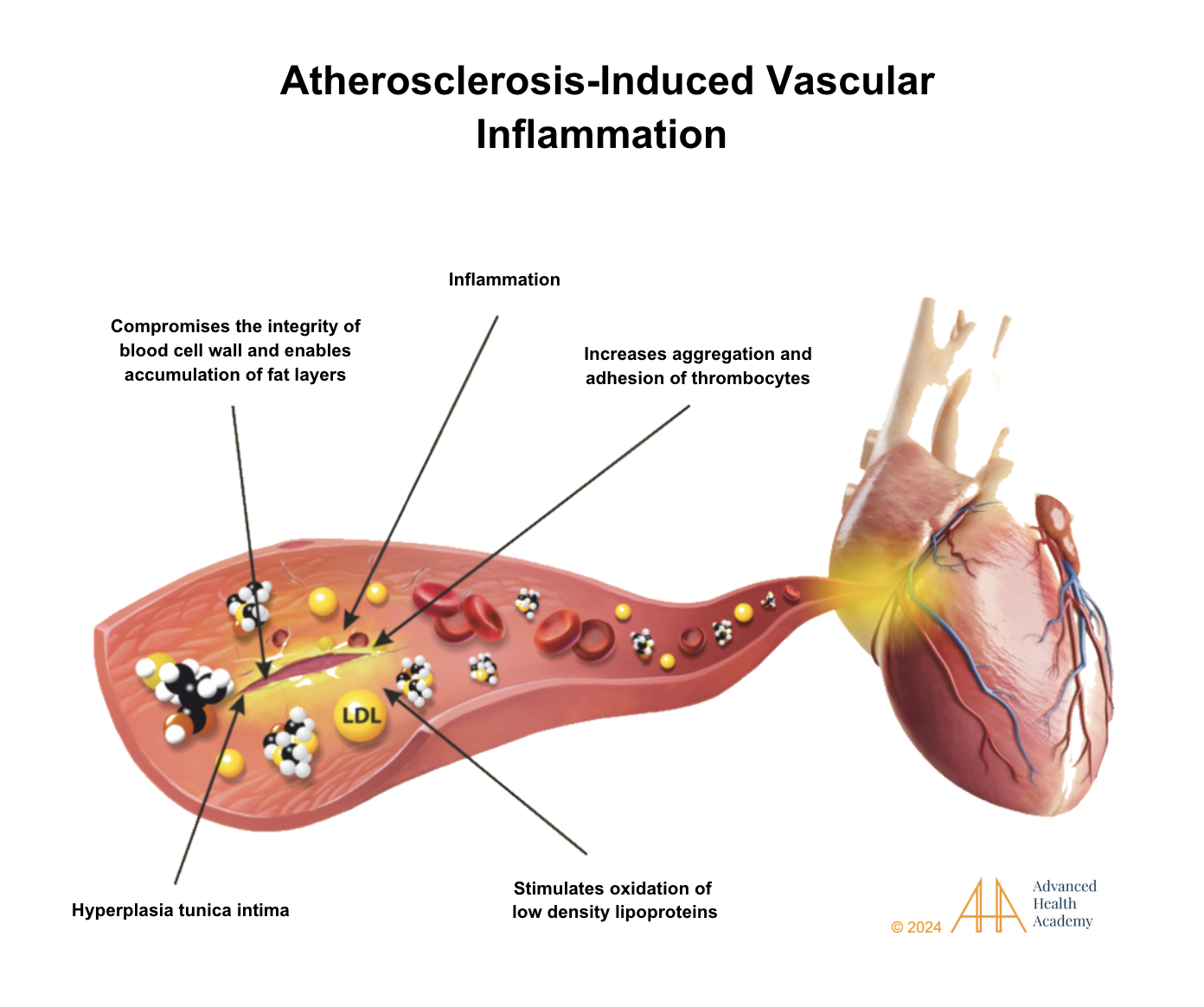
Figure 5: Atherosclerosis is the hardening of arteries due to plaque buildup from excess fat and scar tissue. This reduces blood flow, raises blood pressure, and causes inflammation. Over time, chronic inflammation can cause organs like the heart and pancreas to enlarge and lose function.
Metabolic and Autoimmune Disorders, Infections, and Cancers
High phosphorus levels (hyperphosphatemia) disrupt energy use, fluid balance, and increase the risk of autoimmune diseases, infections, and cancers. Here’s how:
The liver increases glucose and fat production but prevents fat breakdown, leading to fat storage in organs, blood vessels, and tissues. This process also causes damage by releasing heat and reactive molecules (ROS) that oxidize bad cholesterol (LDL), which then sticks to damaged blood vessels. This triggers an immune response where white blood cells (WBCs) try to repair the damage but release inflammatory proteins that can cause blood vessel thickening (atherosclerosis).
Excess ROS damage cells, change genes, and reduce cell growth, leading to diseases like diabetes, fatty liver, obesity, and heart disease. Heart disease causes poor blood flow, raising blood pressure and limiting organ function. This reduces the absorption of important minerals like phosphorus, further affecting energy and health.
The buildup of waste in the blood overactivates WBCs, making them attack the body’s own tissues, leading to autoimmune diseases such as rheumatoid arthritis, lupus, and multiple sclerosis. These conditions cause organ damage and weaken the immune system.
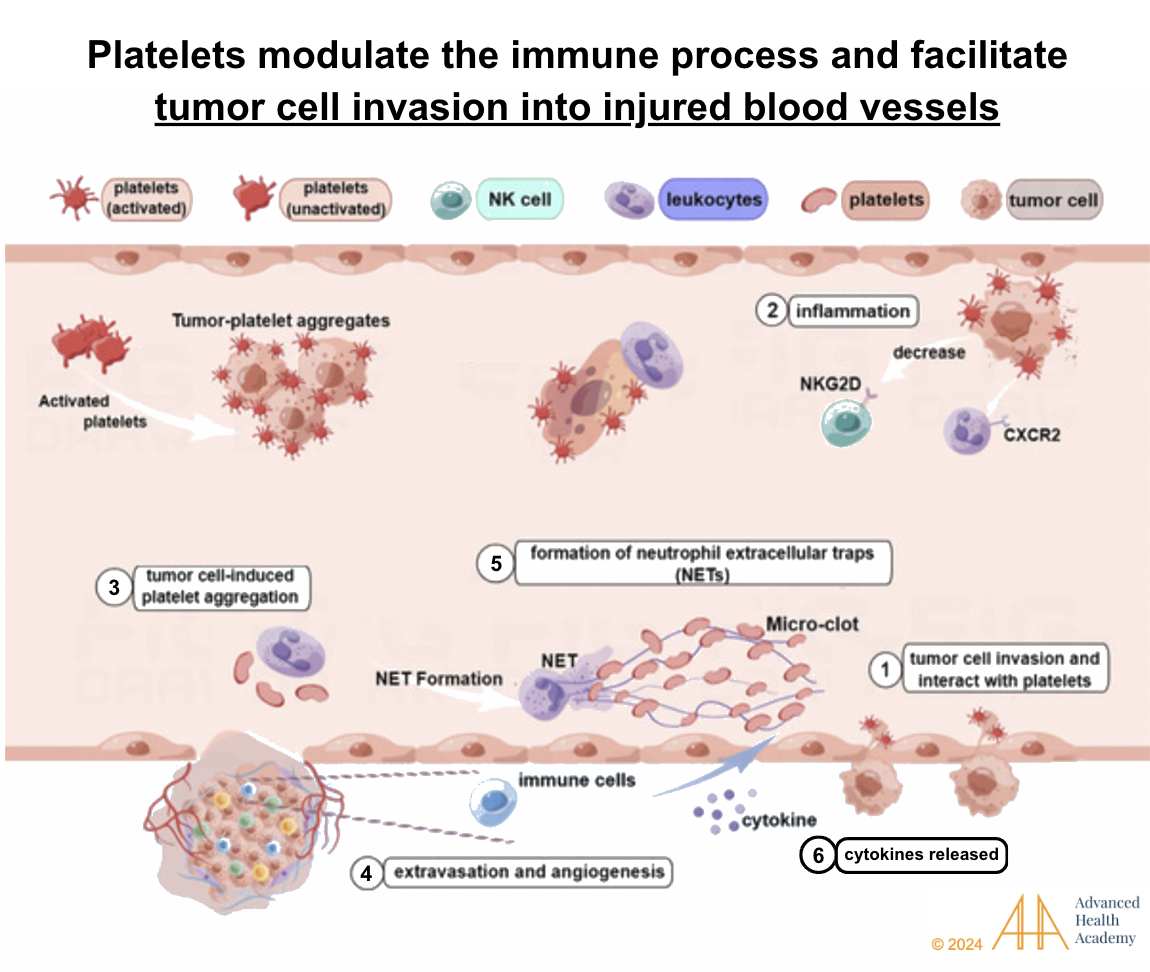
Figure 6: Chronic high phosphate levels can weaken the immune system, raising the risk of heart disease, infections, and cancer. Platelets help cancer cells and pathogens by feeding on iron from damaged cells, which allows them to grow. Neutrophils protect blood vessels but also stop immune cells from attacking tumors and infections. Tumor cells trigger platelets and encourage new blood vessel growth. The immune system’s signals can help pathogens grow, steal nutrients, and spread cancer, contributing to infections and tumor spread.
Chronic high phosphorus levels can increase the risk of many diseases, including autoimmune disorders and cardiovascular diseases, which can lower quality of life. Early detection and treatment are key to managing these health risks.
Kidney Disease
The Kidney International Organization found that high phosphorus levels are common in people with end-stage renal disease (ESRD). Over 60% of hemodialysis patients in the U.S. have phosphorus levels higher than the recommended 5.5 mg/dL. Levels above 6.5 mg/dL increase the risk of death by 27%, partly due to calcium buildup in blood vessels and tissues, which reduces blood flow and speeds up cell damage .
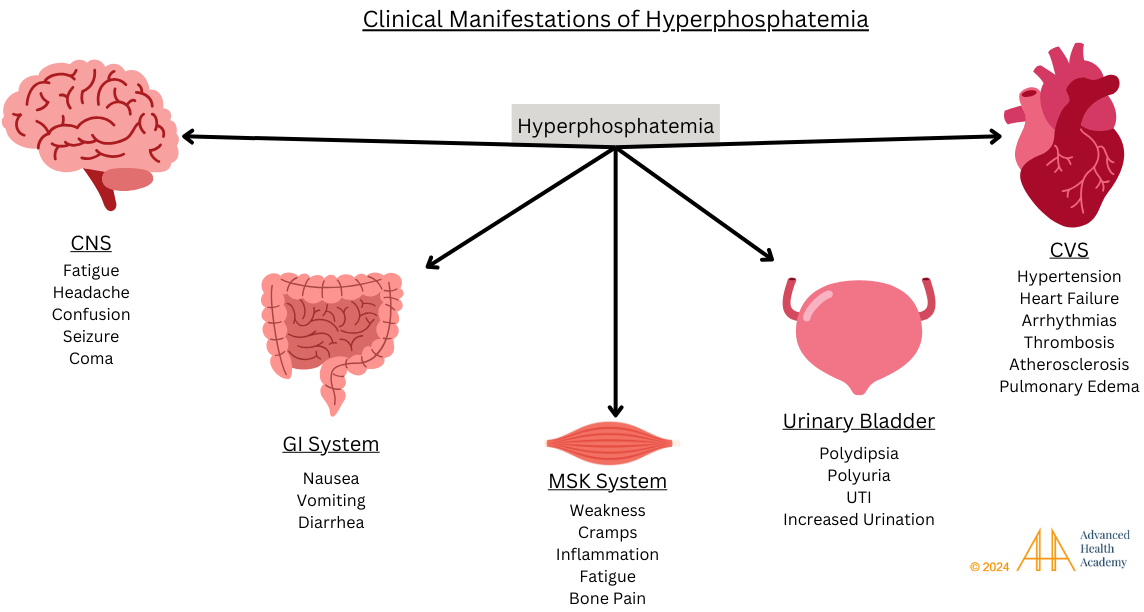
Figure 7: High phosphorus levels (hyperphosphatemia) can harm many organs. In the brain, it may cause confusion or seizures. In the digestive system, it can lead to nausea and diarrhea. Phosphorus imbalances can also cause muscle cramps and bone pain. In the urinary system, it can lead to frequent urination and infections. In the heart, high phosphorus raises blood pressure and increases the risk of heart attacks and strokes.
Clinical Significance of Low Blood Phosphorus Levels
Hypophosphatemia is a condition where phosphorus levels are too low in the blood. Phosphorus is essential for energy production (ATP) and many body functions. Low phosphorus can affect the balance of fluids and electrolytes like magnesium, sodium, and calcium, leading to problems with blood flow, low blood pressure, and strain on organs. For example, it can reduce blood flow to the kidneys, worsening low blood pressure and causing more phosphorus loss in the urine. It also disrupts metabolism, breaks down muscle protein, and slows fat metabolism.
A 1998 study found that 80% of patients with sepsis (blood poisoning) had low phosphorus levels. The inflammation from sepsis causes the body to lose more phosphorus and disrupts how the body handles it. This links high inflammatory markers and low phosphorus in septic patients.
Low phosphorus also affects nerve function, leading to seizures and muscle cramps. It harms bone health by reducing the activity of bone-resorbing cells, which weakens bones and increases the risk of osteoporosis, fractures, and joint problems. It can also cause abnormal calcium levels, leading to hardening of soft tissues and blood vessel stiffness, increasing heart disease risks.
Chronic low phosphorus causes symptoms like fatigue, muscle weakness, bone pain, headaches, and confusion. In severe cases, it can lead to kidney damage, coma, or even sudden death.
Conclusion
Phosphorus is important for energy, bones, fluid balance, and nerve function. Too much or too little can cause joint pain, fatigue, bone issues, and heart problems. It can also affect organs like the heart and kidneys. To keep phosphorus balanced, eat whole plant-based foods, stay hydrated, avoid alcohol and tobacco, manage stress, and get enough sleep. Reducing certain medications also helps. Maintaining healthy phosphorus levels prevents serious health issues like heart attack, stroke, and kidney failure.
Source References and Supplemental Research
Dunn J, Grider MH. Physiology, adenosine triphosphate (ATP). PubMed. Published February 13, 2023. [PubMed]
Vorland CJ, Stremke ER, Moorthi RN, Hill Gallant KM. Effects of Excessive Dietary Phosphorus Intake on Bone Health. Curr Osteoporos Rep. 2017;15(5):473-482. doi:10.1007/s11914-017-0398-4 [PubMed]
National Institutes of Health. Office of Dietary Supplements – Phosphorus. Nih.gov. Published May 4, 2023. [NIH]
Akimbekov, N.S., Digel, I., Sherelkhan, D.K., Razzaque, M.S. (2022). Vitamin D and Phosphate Interactions in Health and Disease. In: Razzaque, M.S. (eds) Phosphate Metabolism . Advances in Experimental Medicine and Biology, vol 1362. Springer, Cham. https://doi.org/10.1007/978-3-030-91623-7_5. [SpringerLink]
Jacquillet, G., Unwin, R.J. Physiological regulation of phosphate by vitamin D, parathyroid hormone (PTH) and phosphate (Pi). Pflugers Arch – Eur J Physiol 471, 83–98 (2019). https://doi.org/10.1007/s00424-018-2231-z. SpringerLink
Prasad N, Bhadauria D. Renal phosphate handling: Physiology. Indian J Endocrinol Metab. 2013;17(4):620-627. doi:10.4103/2230-8210.113752 [PubMed]
Almaden Y, Hernandez A, Torregrosa V, et al. High phosphate level directly stimulates parathyroid hormone secretion and synthesis by human parathyroid tissue in vitro. J Am Soc Nephrol. 1998;9(10):1845-1852. doi:10.1681/ASN.V9101845 [PubMed] [JASN]
Jüppner H. Phosphate and FGF-23. Kidney Int Suppl. 2011;79(121):S24-S27. doi:10.1038/ki.2011.27 [PubMed] [Full Text]
Nadkarni GN, Uribarri J. Phosphorus and the kidney: What is known and what is needed. Adv Nutr. 2014;5(1):98-103. Published 2014 Jan 1. doi:10.3945/an.113.004655 [PubMed]
Hruska KA, Mathew S, Lund R, Qiu P, Pratt R. Hyperphosphatemia of chronic kidney disease. Kidney Int. 2008;74(2):148-157. doi:10.1038/ki.2008.130 [PubMed] [Elsevier] [Full Text]
Ramos AM, Albalate M, Vázquez S, Caramelo C, Egido J, Ortiz A. Hyperphosphatemia and hyperparathyroidism in incident chronic kidney disease patients. Kidney Int Suppl. 2008;(111):S88-S93. doi:10.1038/ki.2008.543 [PubMed] [Elsevier]
Ye G, Yang W, Bi Z, Huang L, Liu F. Effects of a high-phosphorus diet on the gut microbiota in CKD rats. Ren Fail. 2021;43(1):1577-1587. doi:10.1080/0886022X.2021.2003207 [PubMed]
Wu G. Amino acids: metabolism, functions, and nutrition. Amino Acids. 2009;37(1):1-17. doi:10.1007/s00726-009-0269-0 [Pubmed][Crossref]
Jakubowski H., Flatt P. Metabolic Fates of Amino Groups. LibreTexts Biology. [LibreTexts]
Liu, H., Huang, Y., Huang, M. et al. From nitrate to NO: potential effects of nitrate-reducing bacteria on systemic health and disease. Eur J Med Res 28, 425 (2023). https://doi.org/10.1186/s40001-023-01413-y [BMC]
Bryan, N.S., Petrosino, J.F. (2017). Nitrate-Reducing Oral Bacteria: Linking Oral and Systemic Health. In: Bryan, N., Loscalzo, J. (eds) Nitrite and Nitrate in Human Health and Disease. Nutrition and Health. Humana Press, Cham. https://doi.org/10.1007/978-3-319-46189-2_3 [Springer]
Song Y, Liu J, Zhao K, Gao L, Zhao J. Cholesterol-induced toxicity: An integrated view of the role of cholesterol in multiple diseases. Cell Metabolism. 2021;33(10):1911-1925. doi:10.1016/j.cmet.2021.09.001 [Elsevier]
Nordestgaard, B. G., & Varbo, A. (2014). Triglycerides and cardiovascular disease. The Lancet, 384(9943), 626–635. https://doi.org/10.1016/s0140-6736(14)61177-6 [Science Direct] [Scopus] [Google Scholar]
Varbo, A., Benn, M., Tybjærg-Hansen, A., & Nordestgaard, B. G. (2013). Elevated remnant cholesterol causes both Low-Grade inflammation and ischemic heart disease, whereas elevated Low-Density lipoprotein cholesterol causes ischemic heart disease without inflammation. Circulation, 128(12), 1298–1309. https://doi.org/10.1161/circulationaha.113.003008 [Scopus] [Google Scholar]
What Is Gut Dysbiosis? Cleveland Clinic. [Cleveland Clinic]
Adiels M, Olofsson SO, Taskinen MR, Borén J. Overproduction of very low-density lipoproteins is the hallmark of the dyslipidemia in the metabolic syndrome. Arterioscler Thromb Vasc Biol. 2008;28(7):1225-1236. doi:10.1161/ATVBAHA.107.160192 [PubMed] [Full Text] [AHA Journals]
Hansson GK, Hermansson A. The immune system in atherosclerosis. Nat Immunol. 2011;12:204–12. [PubMed] [Crosslink]. Cited by: Herrero-Cervera, A., Soehnlein, O. & Kenne, E. Neutrophils in chronic inflammatory diseases. Cell Mol Immunol. 2022;19(2):177-191. doi:10.1038/s41423-021-00832-3 [PubMed] [PMC Full Text] [Crosslink]
Wilson J.G., Lindquist J.H., Grambow S.C., Crook E.D., Maher J.F. Potential role of increased iron stores in diabetes. Am. J. Med. Sci. 2003;325:332–339. doi: 10.1097/00000441-200306000-00004. [PubMed] [CrossRef] [Google Scholar]
Tiedge M., Lortz S., Drinkgern J., Lenzen S. Relation between antioxidant enzyme gene expression and antioxidative defense status of insulin-producing cells. Diabetes. 1997;46:1733–1742. doi: 10.2337/diab.46.11.1733. [PubMed] [CrossRef] [Google Scholar]
Crawford JH, Chacko BK, Kevil CG, Patel RP. The red blood cell and vascular function in health and disease. Antioxidants & redox signaling. 2004;6(6):992–999. [PubMed] [Google Scholar]
Della Corte V, Todaro F, Cataldi M, Tuttolomondo A. Atherosclerosis and Its Related Laboratory Biomarkers. Int J Mol Sci. 2023;24(21):15546. Published 2023 Oct 24. doi:10.3390/ijms242115546 [PMC Full Text]
Michel JB, Martin-Ventura JL. Red Blood Cells and Hemoglobin in Human Atherosclerosis and Related Arterial Diseases. Int J Mol Sci. 2020;21(18):6756. Published 2020 Sep 15. doi:10.3390/ijms21186756 [PMC Full Text]
Chen, L., Deng, H., Cui, H., Fang, J., Zuo, Z., Deng, J., Li, Y., Wang, X., & Zhao, L. (2017). Inflammatory responses and inflammation-associated diseases in organs. Oncotarget, 9(6), 7204–7218. [Oncotarget] [Crosslink]
Godkin A, Smith KA. Chronic infections with viruses or parasites: breaking bad to make good. Immunology. 2017;150(4):389-396. doi:10.1111/imm.12703 [Pubmed] [Crossref]
Hom J, Dulmovits BM, Mohandas N, Blanc L. The erythroblastic island as an emerging paradigm in the anemia of inflammation. Immunologic Research. 2015;63(1-3):75-89. doi:https://doi.org/10.1007/s12026-015-8697-2 [Springer]
Conigliaro, P., Chimenti, Triggianese, P., Sunzini, F., Novelli, L., Perricone, C., & Perricone, R. (2016). Autoantibodies in inflammatory arthritis. Autoimmunity Reviews, 15(7), 673–683. https://doi.org/10.1016/j.autrev.2016.03.003 [Science Direct]
Feingold, K. R., & Grunfeld, C. (2022, March 7). The effect of inflammation and infection on lipids and lipoproteins. Endotext – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK326741/ [NIH]
Mrabet, S., Wafa, M., & Giovannoni, G. (2022). Multiple sclerosis and migraine: Links, management and implications. Multiple Sclerosis and Related Disorders, 68, 104152. https://doi.org/10.1016/j.msard.2022.104152 [Science Direct]
Avina-Zubieta JA, Choi HK, Sadatsafavi M, Etminan M, Esdaile JM, Lacaille D. Risk of cardiovascular mortality in patients with rheumatoid arthritis: a meta-analysis of observational studies. Arthritis Rheum. 2008;59:1690–1697. [PubMed] [Reference list]
Lindhardsen J, Ahlehoff O, Gislason GH, Madsen OR, Olesen JB, Torp-Pedersen C, Hansen PR. The risk of myocardial infarction in rheumatoid arthritis and diabetes mellitus: a Danish nationwide cohort study. Ann Rheum Dis. 2011;70:929–934. [PubMed] [Reference list]
Redirecting. Doi.org. Published 2024. Accessed September 25, 2024. https://doi.org/10.1111/j.1523-1755.2004.09004.x [Kidney International] [ScienceDirect]
Nanji AA, Freeman HJ. Postural hypotension and labile blood pressure associated with severe hypophosphatemia. Int J Cardiol. 1984;5(3):379-381. doi:10.1016/0167-5273(84)90118-9 [PubMed] [Elsevier]
Barak V, Schwartz A, Kalickman I, Nisman B, Gurman G, Shoenfeld Y. Prevalence of hypophosphatemia in sepsis and infection: the role of cytokines. Am J Med. 1998;104(1):40-47. doi:10.1016/s0002-9343(97)00275-1 [PubMed] [Elsevier]
Rroji M, Figurek A, Viggiano D, Capasso G, Spasovski G. Phosphate in the Context of Cognitive Impairment and Other Neurological Disorders Occurrence in Chronic Kidney Disease. Int J Mol Sci. 2022;23(13):7362. Published 2022 Jul 1. doi:10.3390/ijms23137362 [PubMed]
Khan M, Jose A, Sharma S. Physiology, Parathyroid Hormone. [Updated 2022 Oct 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: [PubMed]
Day AL, Morgan SL, Saag KG. Hypophosphatemia in the setting of metabolic bone disease: case reports and diagnostic algorithm. Ther Adv Musculoskelet Dis. 2018;10(7):151-156. doi:10.1177/1759720X18779761 [PubMed]
Voelkl J, Egli-Spichtig D, Alesutan I, Wagner CA. Inflammation: a putative link between phosphate metabolism and cardiovascular disease. Clin Sci (Lond). 2021;135(1):201-227. doi:10.1042/CS20190895 [PubMed]
Alexander J, Nagi D. Isolated hypophosphataemia as an early marker of primary hyperparathyroidism. Endocrinol Diabetes Metab Case Rep. Published online June 1, 2021. doi:10.1530/EDM-20-0217 [PubMed]
Romagnoli C, Iantomasi T, Brandi ML. Impact of X-Linked Hypophosphatemia on Muscle Symptoms. Genes (Basel). 2022;13(12):2415. Published 2022 Dec 19. doi:10.3390/genes13122415 [PubMed]
Little R, Ellison DH. Modifying Dietary Sodium and Potassium Intake: An End to the ‘Salt Wars’?. Hypertension. 2024;81(3):415-425. doi:10.1161/HYPERTENSIONAHA.123.19487 [PubMed] [Full Text]
Zarantonello D, Brunori G. The Role of Plant-Based Diets in Preventing and Mitigating Chronic Kidney Disease: More Light than Shadows. J Clin Med. 2023;12(19):6137. Published 2023 Sep 22. doi:10.3390/jcm12196137 [PubMed]
Jardine MA, Kahleova H, Levin SM, Ali Z, Trapp CB, Barnard ND. Perspective: Plant-Based Eating Pattern for Type 2 Diabetes Prevention and Treatment: Efficacy, Mechanisms, and Practical Considerations. Adv Nutr. 2021;12(6):2045-2055. doi:10.1093/advances/nmab063 [PubMed]
Bosman A, Campos-Obando N, de Keyser CE, Stricker BH, Zillikens MC. Diuretic Use and Serum Phosphate: Rotterdam Study and UK Biobank. J Endocr Soc. 2024;8(5):bvae057. Published 2024 Mar 25. doi:10.1210/jendso/bvae057 [PubMed]
Kennedy M. How much water you’re actually supposed to drink each day – and why 8 cups isn’t right for everyone. Business Insider. December 14, 2021. [Website]
National Research Council (US) Subcommittee on the Tenth Edition of the Recommended Dietary Allowances. Recommended Dietary Allowances: 10th Edition. Washington (DC): National Academies Press (US); 1989. 11, Water and Electrolytes. Available from: [PubMed]
Davis RF, Eichner JM, Bleyer WA, Okamoto G. Hypocalcemia, hyperphosphatemia, and dehydration following a single hypertonic phosphate enema. J Pediatr. 1977;90(3):484-485. doi:10.1016/s0022-3476(77)80723-3 [PubMed] [Elsevier]
Baj J, Flieger W, Teresiński G, et al. Magnesium, Calcium, Potassium, Sodium, Phosphorus, Selenium, Zinc, and Chromium Levels in Alcohol Use Disorder: A Review. J Clin Med. 2020;9(6):1901. Published 2020 Jun 18. doi:10.3390/jcm9061901 [PubMed]
Amstrup AK, Rejnmark L, Vestergaard P, Heickendorff L, Mosekilde L. Effects of smoking on severity of disease in primary hyperparathyroidism. Calcif Tissue Int. 2010;87(5):406-413. doi:10.1007/s00223-010-9416-6 [PubMed] [SpringerLink]
Lee J, Taneja V, Vassallo R. Cigarette smoking and inflammation: cellular and molecular mechanisms. J Dent Res. 2012;91(2):142-149. doi:10.1177/0022034511421200 [PubMed]
Oakes JM, Fuchs RM, Gardner JD, Lazartigues E, Yue X. Nicotine and the renin-angiotensin system. Am J Physiol Regul Integr Comp Physiol. 2018;315(5):R895-R906. doi:10.1152/ajpregu.00099.2018 [PubMed]
Li J, Wang L, Han M, et al. The role of phosphate-containing medications and low dietary phosphorus-protein ratio in reducing intestinal phosphorus load in patients with chronic kidney disease. Nutr Diabetes. 2019;9(1):14. Published 2019 Apr 3. doi:10.1038/s41387-019-0080-2 [PubMed]
Megapanou E, Florentin M, Milionis H, Elisaf M, Liamis G. Drug-Induced Hypophosphatemia: Current Insights. Drug Saf. 2020;43(3):197-210. doi:10.1007/s40264-019-00888-1 [PubMed][SpringerLink]
Ray EC, Rondon-Berrios H, Boyd CR, Kleyman TR. Sodium Retention and Volume Expansion in Nephrotic Syndrome: Implications for Hypertension. Advances in Chronic Kidney Disease. 2015;22(3):179-184. doi:https://doi.org/10.1053/j.ackd.2014.11.006 [Elsevier]
Ge D, Su S, Zhu H, et al. Stress-induced sodium excretion: a new intermediate phenotype to study the early genetic etiology of hypertension?. Hypertension. 2009;53(2):262-269. doi:10.1161/HYPERTENSIONAHA.108.118117 [PubMed]
Knutson KL. Impact of sleep and sleep loss on glucose homeostasis and appetite regulation. Sleep Med Clin. 2007;2(2):187-197. doi:10.1016/j.jsmc.2007.03.004 [PubMed]
Hirshkowitz M, Whiton K, Albert SM, et al. National Sleep Foundation’s sleep time duration recommendations: methodology and results summary. Sleep Health. 2015;1(1):40-43. doi:10.1016/j.sleh.2014.12.010 [PubMed] [Elsevier]
Hamasaki H. The Effects of Mindfulness on Glycemic Control in People with Diabetes: An Overview of Systematic Reviews and Meta-Analyses. Medicines (Basel). 2023;10(9):53. Published 2023 Sep 7. doi:10.3390/medicines10090053 [PubMed]
Pascoe MC, Thompson DR, Jenkins ZM, Ski CF. Mindfulness mediates the physiological markers of stress: Systematic review and meta-analysis. J Psychiatr Res. 2017;95:156-178. doi:10.1016/j.jpsychires.2017.08.004 [PubMed] [Elsevier]