ALT and AST: Alanine Aminotransferase and Aspartate Aminotransferase: Diagnostic Significance and Clinical Insights
Authors: Payal Bhandari M.D., Amer Džanković, Madison Granados
Contributors: Vivi Chador, Hailey Chin, Nigella Umali Ruguian
Key Insights
The liver, known as the body’s “chemical factory,” is essential for metabolism, detoxification, energy, blood clotting, and immune function. Liver function tests, including ALT, AST, alkaline phosphatase, albumin, bilirubin, and GGT, assess liver health1,2.
ALT is specific to the liver, while AST is also found in the heart, muscles, brain, and lungs3.Elevated levels indicate liver damage, often caused by medications, steroids, creatine supplements4, or substances like alcohol and tobacco, which can harm liver function over time5. Conditions like hepatitis, NAFLD, and steatohepatitis may go unnoticed until severe stages like cirrhosis.
ALT and AST tests are crucial for detecting liver damage, guiding treatment, and advancing research.
What are ALT and AST?
Enzymes are proteins that speed up metabolic processes like tissue building, substance transport, and chemical reactions. Alanine aminotransferase (ALT or SGPT) and aspartate aminotransferase (AST or SGOT) are key enzymes involved in amino acid metabolism2. Enzymes bind to specific molecules, or substrates, reducing the energy required for reactions. Without them, essential processes like digestion, DNA replication, and muscle or nerve function would be too slow to sustain life. Despite their varied roles, enzymes share chemical features critical to their function.
Amino Acids are the Building Blocks of Protein
Proteins are made of amino acids, the building blocks of life. Each amino acid has an amino group (-NH2), carboxyl group (-COOH), and unique side chain (R). Of the 20 amino acids essential for protein synthesis, some must be obtained from food. Amino acids link via peptide bonds into chains, with their sequence determining protein shape and function. Even minor changes can impact function, causing diseases or enhancing activity.5, 6,7
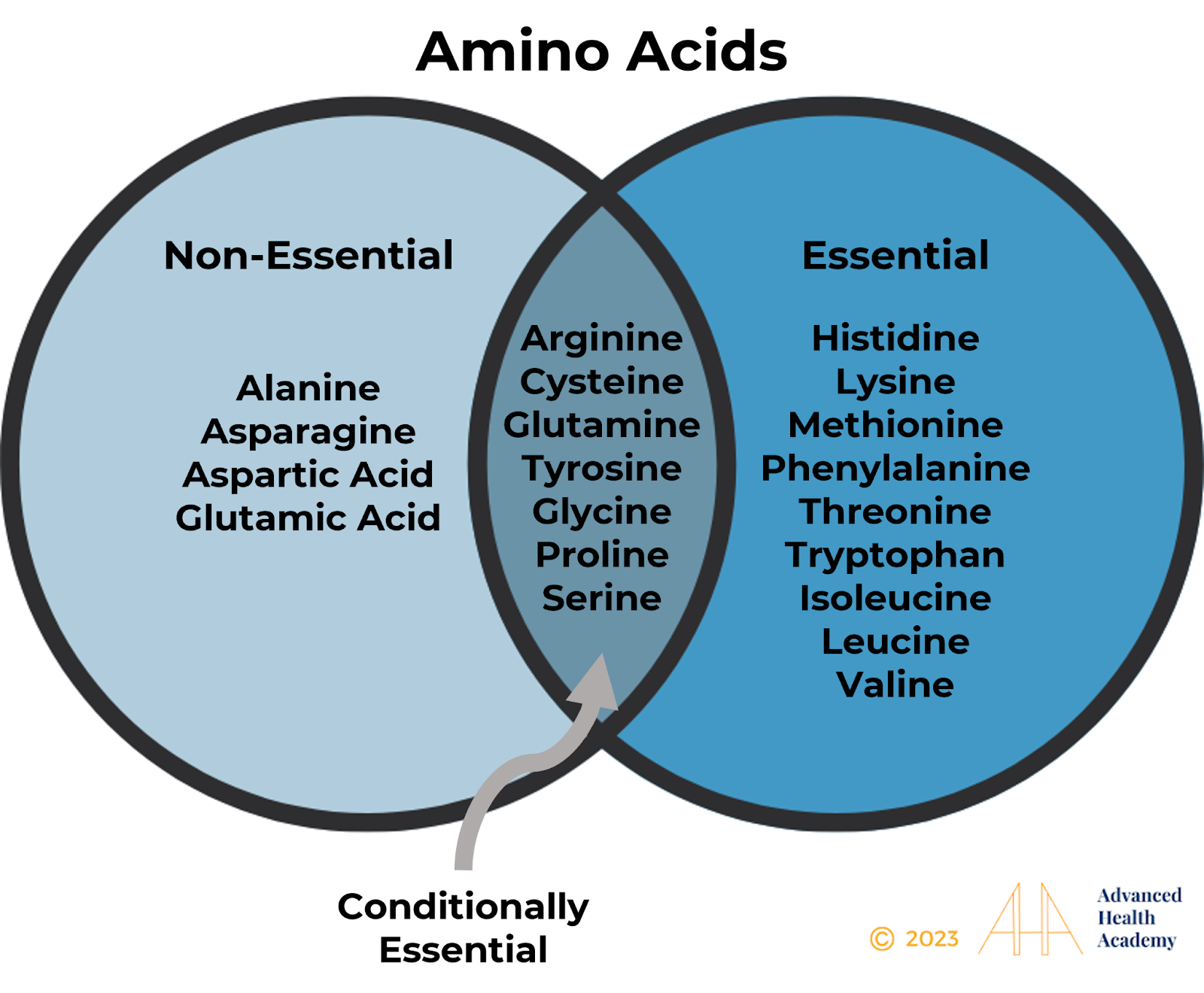
Figure 1: The amino acids.
Protein Metabolism and Synthesis
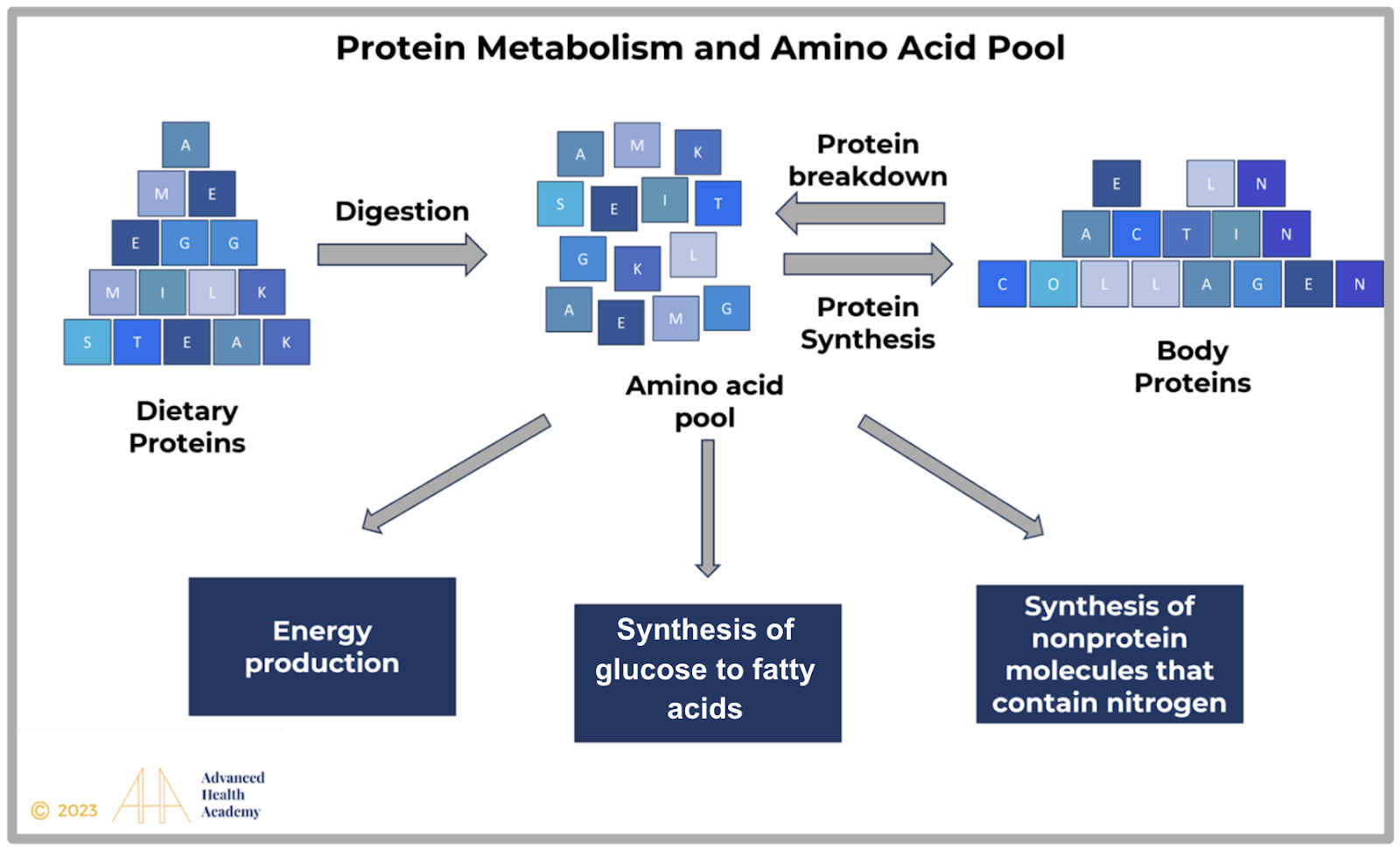
Figure 2: Protein cannot be stored and is broken into amino acids for new proteins, nonessential amino acids, and nitrogen compounds. Excess protein converts to glycogen or fat for energy or metabolic pathways.
Role of AST and ALT in the Body
The body usually gets energy (ATP) from glucose in food. However, during long periods without eating, intense exercise, insulin deficiency (like in diabetes), or when the brain needs extra energy, the body breaks down fats and proteins into amino acids, lactate, and glycerol for fuel. This process, called ketogenesis, happens mainly in the liver and partly in the kidneys and small intestine. Because the brain can’t use fat directly for energy, the glycerol from fats must be turned into glucose through a process called gluconeogenesis.
Harvesting Energy (ATP) After A Meal
Food is digested in the small intestine, releasing glucose, fatty acids (FAs), and amino acids (AAs) into the blood. Insulin moves glucose to tissues for energy (ATP), while excess nutrients are processed in the liver. Glucose is stored as glycogen or converted into FAs and AAs. FAs form triacylglycerol (TAG), stored or released as VLDL. Proteins and AAs are used for energy, protein synthesis, or glucose production, with toxic byproducts detoxified.
Harvesting Energy During Short-Term Fasting, Intense Exercise, and Emotional Intensity
Gluconeogenesis reduces oxaloacetate in liver cells, blocking acetyl-CoA from entering the Krebs cycle. To compensate, glucagon and epinephrine lower insulin and activate lipoprotein lipase (LPL), which breaks down glycogen and fats. This releases acetyl-CoA, converted into acetoacetate for energy (ATP) or beta-hydroxybutyrate. Some acetoacetate becomes acetone, exhaled through the lungs .
Harvesting Energy During Prolonged Fasting
During starvation or intense exercise, the body shifts to alternative energy sources. The liver releases VLDL cholesterol, fat tissue breaks down fatty acids and glycerol for ketones, and muscles break down proteins, releasing lactate and alanine. The liver converts these into glucose through gluconeogenesis, involving lactate oxidation to pyruvate and cycles through oxaloacetate and malate.
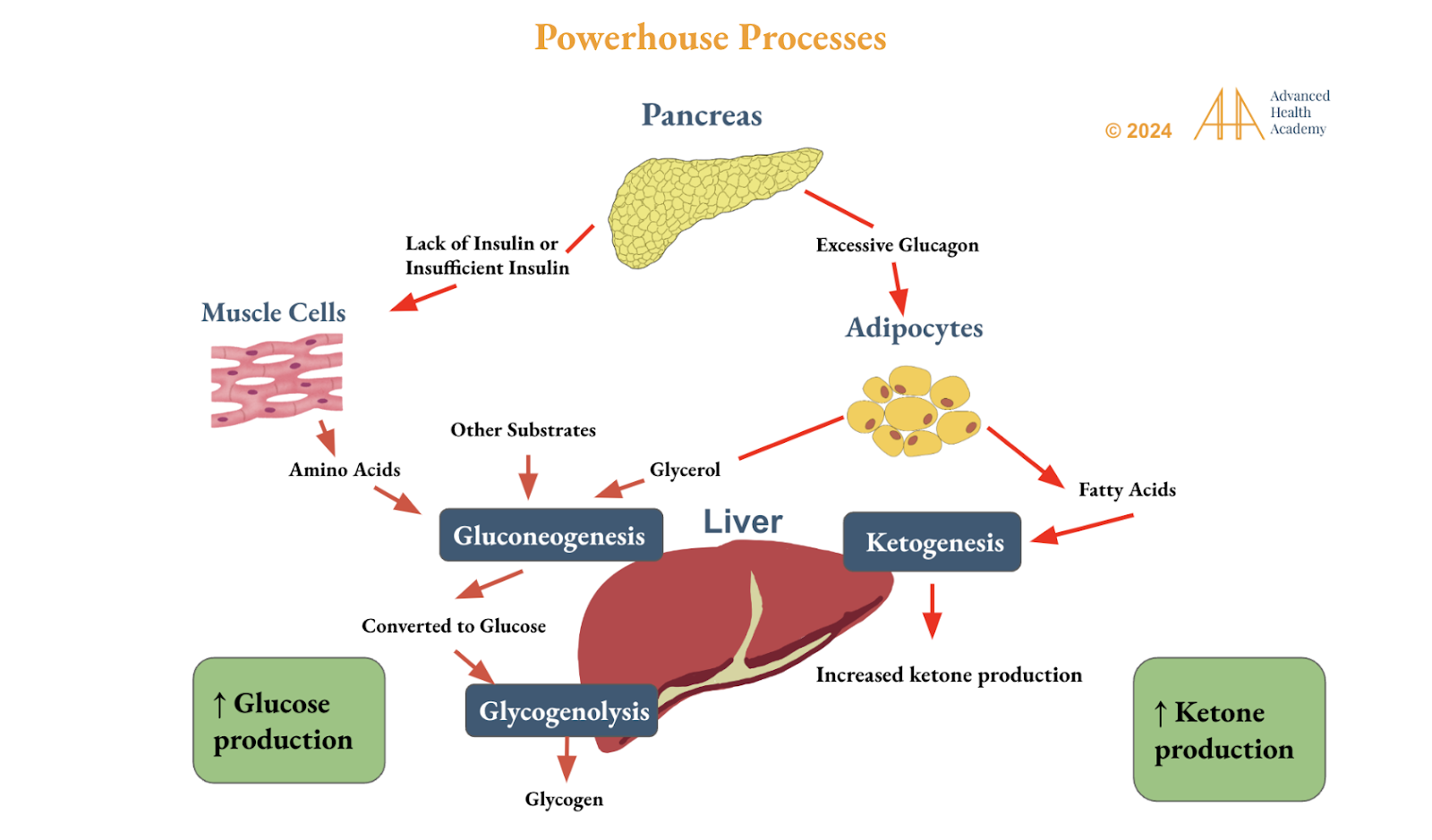
Figure 3: Circadian rhythm genes regulate liver glucose and ketone production for energy. During fasting or exercise, ketones stabilize blood sugar, improve insulin sensitivity, and reduce reliance on carbs, lowering hunger, anxiety, inflammation, and stress hormones.
The Synthesis and Metabolism of Amino Acids
Amino acids break down into intermediates for the Krebs Cycle to produce energy. Glucogenic amino acids form pyruvate, while ketogenic ones produce acetyl-CoA and ketones. Non-essential amino acids are made through protein breakdown, transamination, and nitrogen removal (deamination) 6, 11.
Glutamic acid/glutamate (Glu), glutamine (Gln), and alanine (Ala) are the most abundant amino acids in the body and an integral part of human cells and bacterial cell walls.11 They play unique roles in protein metabolism, cell signaling, harvesting energy, and nitrogen homeostasis. Glu and Gln are the primary sources of ammonium production in cells.
Glu is most abundant in the liver, kidneys, and muscles. It is the brain’s main excitatory chemical, helping neurons and astrocytes send signals to communicate. Glu plays a key role in learning, memory, and adapting connections in the brain.
The small intestine metabolizes 90% of Glu into amino acids like alanine, proline, aspartate, and citrulline12, leaving little Glu in the blood after meals13.
Glu cannot cross the blood-brain barrier and is converted in the brain to GABA, an inhibitory neurotransmitter that regulates neural activity, sleep, mood, pain relief, and blood pressure15,16,17
Aspartate/aspartic acid is a powerful antioxidant in the nervous, endocrine, and reproductive systems.18 It supports the synthesis and release of hormones like glucocorticoids, prolactin, oxytocin, and steroids.19
ALT and AST are essential for amino acid conversion and metabolite production. AST produces oxaloacetate and glutamate, which support energy production in the Krebs cycle. ALT deaminates alanine, creating pyruvate, which is used to make glucose through gluconeogenesis. ALT helps regulate blood sugar, especially during fasting and intense exercise.
Degradation of Toxic Nitrogen
In the liver, toxic amino groups (-NH2) from amino acid metabolism are converted to ammonia, then to less toxic urea with carbon dioxide released. About 40-50% of urea is excreted by the kidneys in urine, and 10% is eliminated through sweat, stool, and breath20. The remaining urea is either stored as fat in the liver, abdomen, and muscles or accumulates in the blood, causing cell damage.
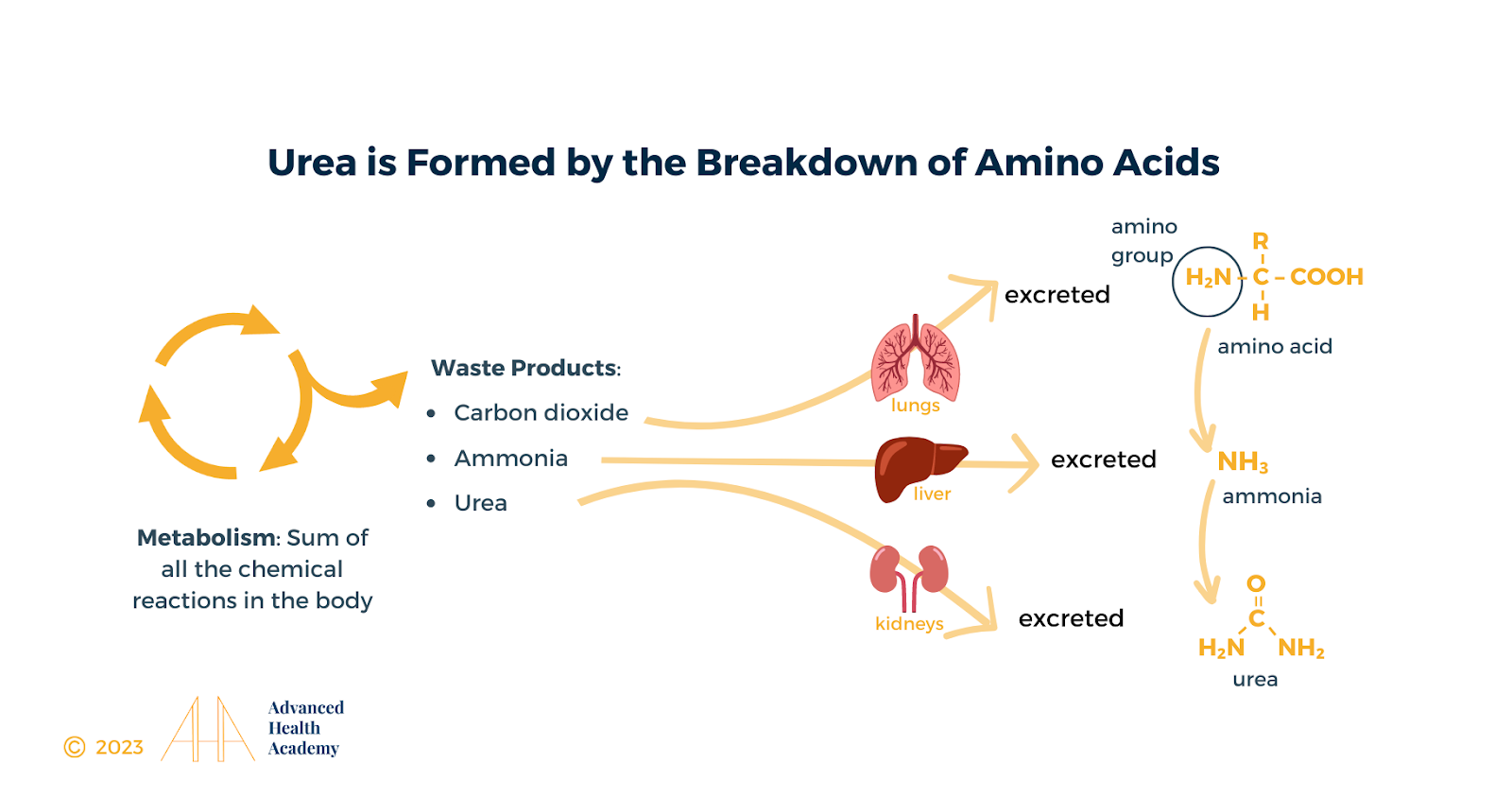
Figure 4: The toxic amino group derived from metabolizing amino acids are broken into the urea, ammonia, and carbon dioxide, and subsequently either excreted in the urine and during exhalation, or recycled in the liver.
Regulation of AST and ALT Synthesis
Hormonal Regulation:
Hormones such as insulin and glucagon can influence the synthesis of AST and ALT. For example, glucagon stimulates gluconeogenesis, which can upregulate ALT activity in the liver.
Nutritional Status:
Amino acid levels and nutritional status influence enzyme activity. During fasting or starvation, the body boosts gluconeogenesis, which increases ALT activity.
Cellular Stress and Damage:
Cell stress or damage increases AST and ALT production. When liver cells are damaged, these enzymes are released into the blood, raising transaminase levels detectable in tests.
Clinical Significance of Monitoring AST and ALT Levels
Non-alcoholic fatty liver disease (NAFLD) is a leading cause of abnormal transaminase levels and metabolic issues. There is no effective drug to treat this widespread condition. Figure 6 shows that poor liver function is linked to reduced blood flow to the digestive organs, slowing digestion and causing gut bacteria imbalance (dysbiosis). Gut microbiota aids in digestion, nutrient absorption, and waste removal.
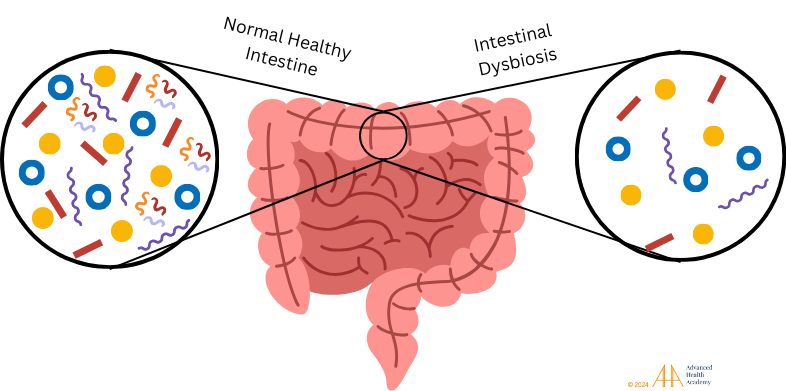
Figure 5: Healthy gut microbiota support digestion, nutrient absorption, and waste removal. Dysbiosis disrupts metabolism, increases harmful pathogens, and weakens immune responses177.
Dysbiosis allows undigested food into the bloodstream, thickening blood, reducing oxygen (hypoxia), and causing cell death, inflammation, and ROS. It lowers RBC production, prompting kidneys to release erythropoietin, while WBCs clear debris, form clots, and create vessels. This leads to atherosclerosis, disrupting energy and linking elevated transaminase to inflammation, autoimmune disorders, and organ damage.
Elevated AST and ALT indicate liver, bile duct, or gallbladder dysfunction and may affect the heart, pancreas, or kidneys. Changes in bilirubin and alkaline phosphatase can reveal metabolic issues. ALT is more specific to liver disorders, and the AST/ALT ratio aids diagnosis25.
ALT Elevation is Greater Than Elevated or Normal AST
In acute liver inflammation, ALT and AST levels can rise significantly due to infection, medications, or stress. Mild elevations (2-3 times normal) often result from protein metabolism issues. NAFLD, the leading cause of elevated ALT-to-AST ratios globally26, includes steatosis, NASH, fibrosis, and cirrhosis. It is linked to fat storage, insulin resistance, and diabetes27,28,29. Abdominal fat is a stronger predictor of elevated ALT than body weight, as shown in studies with over 17,000 participants. 30,31,32,33,34,35,36,37
Elevated AST Alone
Elevated AST levels alone suggest increased glutamate and aspartate processing, leading to higher levels of these amino acids in the blood and triggering an immune response.
Elevated ALT Level Alone
Sudden weight loss and prolonged fasting can raise ALT levels mildly (2–3 times normal), while starvation, such as in anorexia nervosa, can increase them significantly (4–30 times normal)38. Low RBC and hemoglobin levels reduce oxygen delivery (hypoxia), causing RBC destruction (hemolysis) and releasing toxic byproducts processed by the liver and spleen. Excess hemolysis increases bilirubin processing, often leading to gallstones. A study found ALT levels at 82.5 IU/L in cholecystitis patients without gallstones and 95 IU/L in those with gallstones39. Gallstone-induced pancreatic inflammation raised ALT to about 200 IU/L42.Excess bilirubin can cross the blood-brain barrier, damaging nerve cells and affecting vision, speech, cognition, hormones, and electrolyte balance35, 43,44, 45, 46, 47.
AST Elevation Is Greater Than Elevated or Normal ALT
The primary causes of higher AST levels in comparison to the ALT levels include, but are not limited to, the following:
Alcohol can damage genes for enzymes like alcohol dehydrogenase, aldehyde dehydrogenase, and cytochrome P450 2E1, leading to higher acetaldehyde and estrogen levels in tissues and blood48,49,50. Acetaldehyde harms liver cell structure and function, causing:
Decreased metabolism of amino acids and synthesis of many proteins (such as hemoglobin and red blood cells)
Dysregulated gluconeogenesis and ketogenesis, and increased fat storage51
Dysregulated hormonal and energy homeostasis
Accelerated red blood cell (RBC) destruction, elevating reactive oxygen species (ROS), altering metabolic pathways, damaging cells in various organs, and increasing AST and ALT levels.
Chronic liver dysfunction and disease is characterized by moderate-to-severe scar tissue deposition that alters its structure and function.86
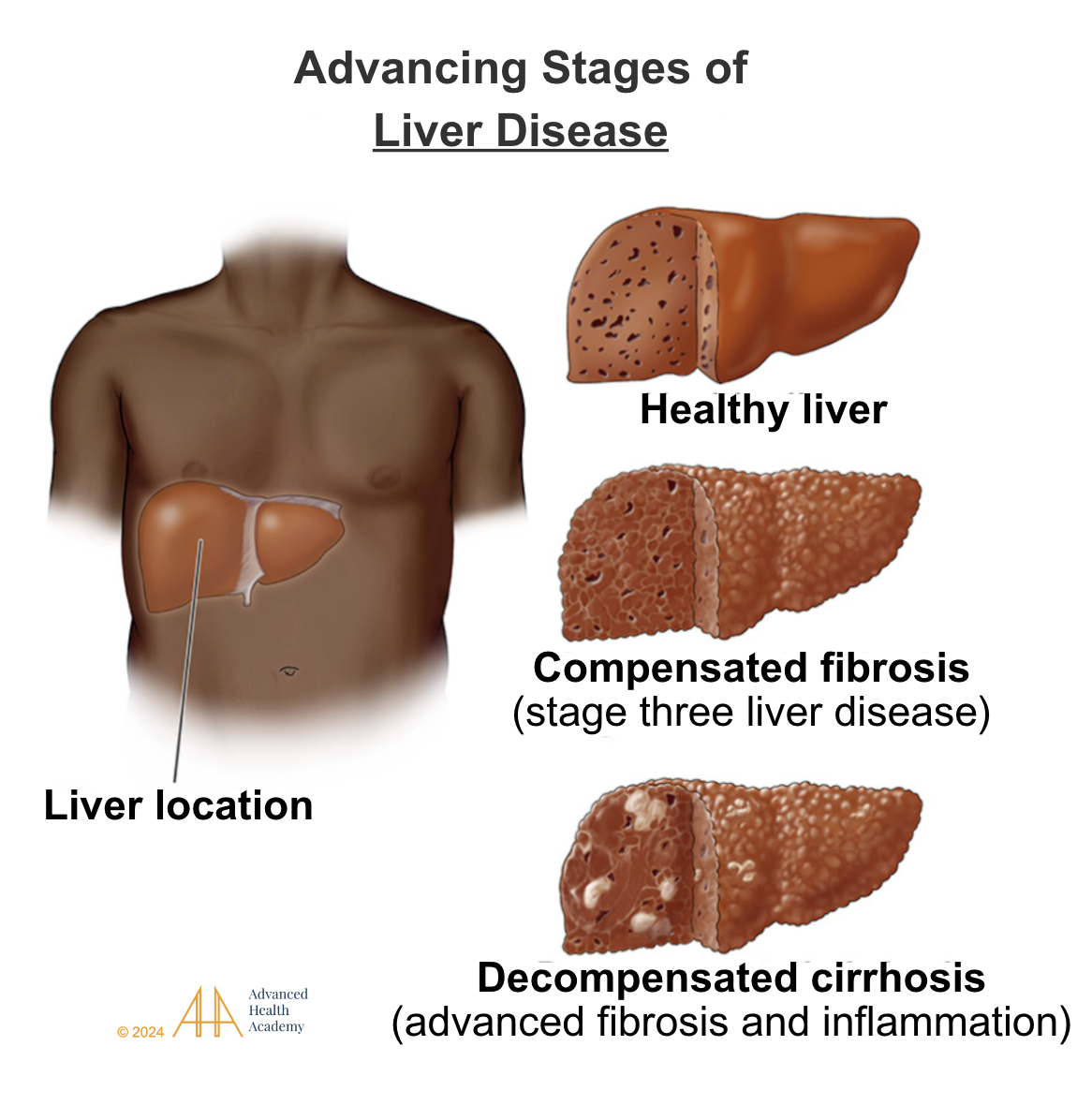
Figure 6: Liver dysfunction triggers inflammation, diverting nutrients from organ functions to toxin removal. Chronic inflammation causes structural damage, scarring, clotting, and liver failure.
Copper is essential for protein metabolism and is stored mainly in bones and muscles54. Wilson disease, an autosomal recessive disorder, causes excess copper to build up in the blood due to a gene mutation56,57,58. Copper toxicity can result from uncoated cookware, contaminated water, or exposure to sources like pesticides and burn creams. Foods rich in copper include animal products, nuts, seeds, and spinach. Low copper intake increases absorption, making accidental exposure more harmful53.
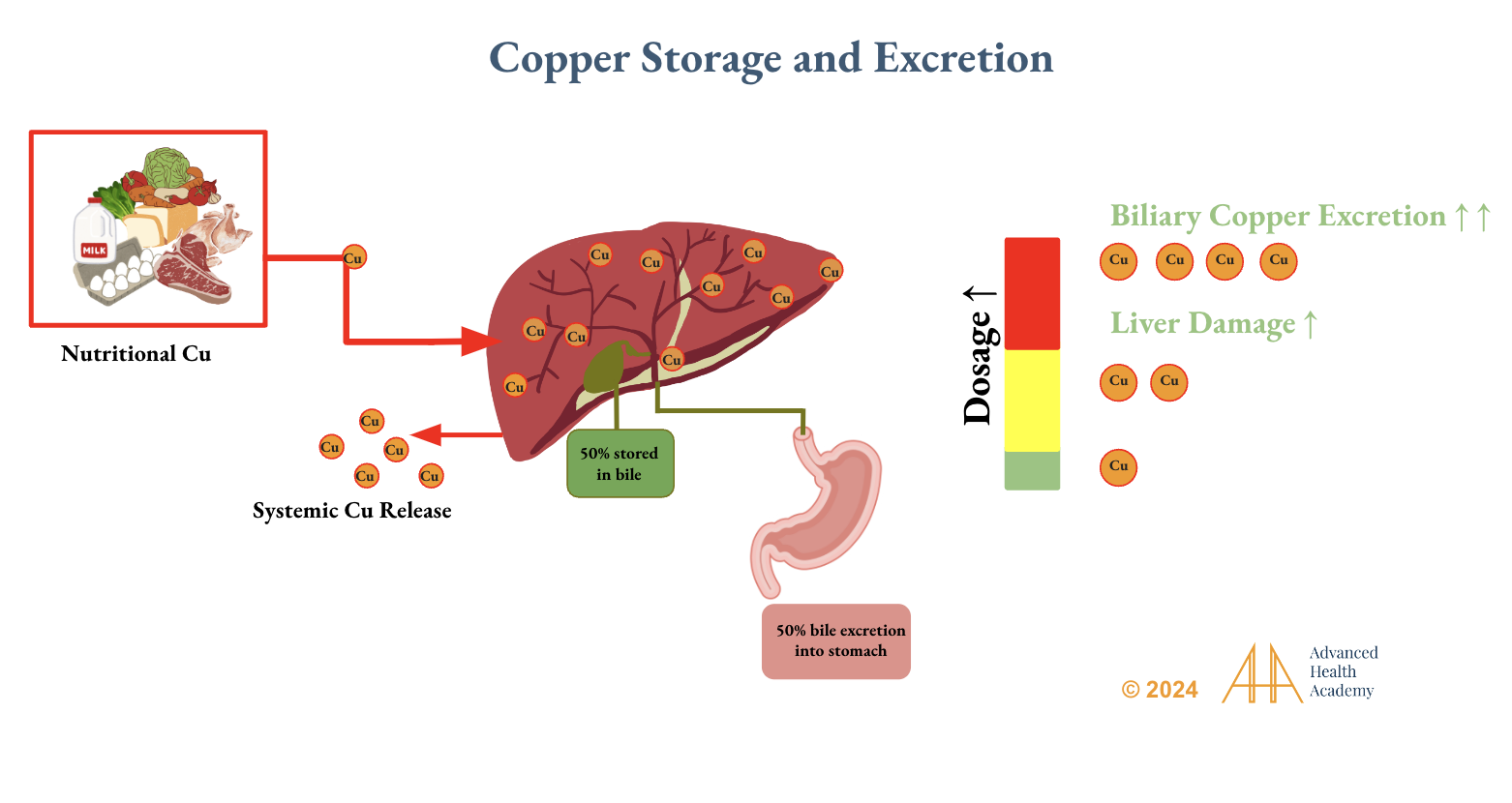
Figure 7: Dietary copper (Cu) is absorbed in the small intestine and transported to the liver, where 85 to 95 percent is bound to the protein ceruloplasmin. 50 percent of copper is stored in the gallbladder as bile, while the remaining is loosely bound to albumin and other small molecules and excreted into the stomach.55 Excess consumption of copper-rich foods (such as animal products) can lead to liver damage and cause excess free copper ions into the circulation.58
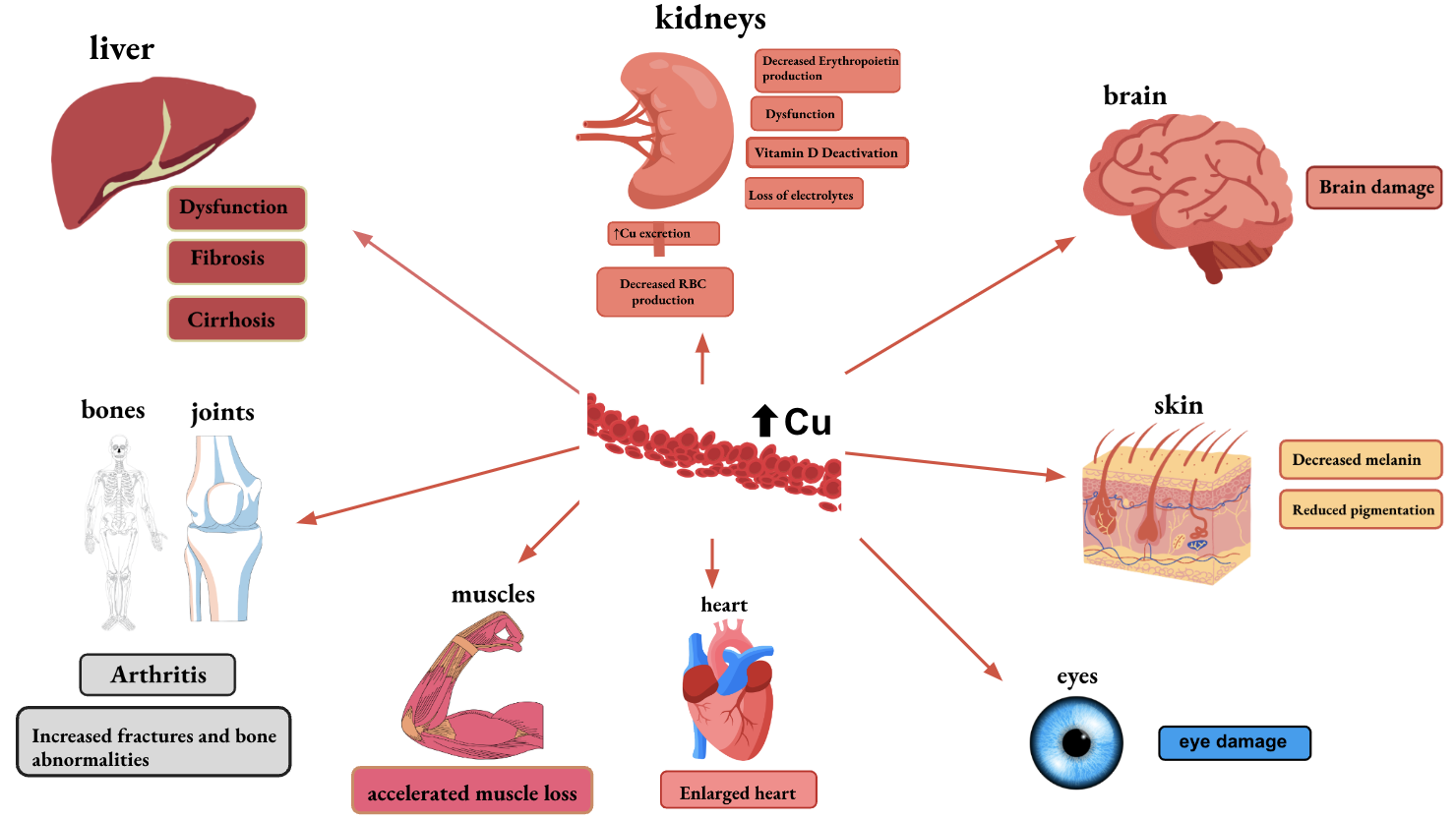
Figure 8: Excess free copper ions in the circulation can damage the structure, function, and genetic code of various organs, decrease red blood cell production, and alter skin pigmentation 56,57,58.
Depressed AST and ALT Levels
Low AST and ALT levels usually indicate good liver function. However, in advanced liver disease (e.g., cirrhosis), they may reflect depleted liver function. Chronic medication use, malnutrition, and frequent nicotine or alcohol use can also lower transaminase levels.
Prevalence and Statistics Regarding Abnormal AST and ALT Levels
Abnormal ALT and AST levels indicate disrupted protein metabolism, leading to toxic free nitrogen, increased reactive oxygen species (ROS), cell damage, and altered metabolic pathways.
Liver disease is rising globally and in the U.S., where it was the 8th leading cause of death in 201661. NAFLD, now the leading cause of liver-related deaths, surpasses viral causes. Diagnosed through imaging or histology, NAFLD results from the liver’s inability to process excess fat and protein. Its severe form, NASH, causes liver cell injury, increasing risks of complications and organ failure. Between 1988 and 2002, ALT levels doubled to 8.9% and AST to 4.9%, with NAFLD prevalence in the U.S. matching the global rate of 25.24%62, 63.
NAFLD and abnormal ALT/AST levels are influenced by socioeconomic, ethnic, and genetic factors. Hispanic Americans have higher NAFLD risks, with 33% prevalence in Mexican Americans compared to 16% in Dominicans and 18% in Puerto Ricans. A mutation in the PNPLA3 gene, which produces adiponutrin, is a key genetic risk factor65.
Although genetics cannot be changed, healthier lifestyle choices, including diet and exercise, can significantly improve liver health and reduce disease risks.
Conclusion
Alanine aminotransferase (ALT) and aspartate aminotransferase (AST) are vital enzymes for amino acid metabolism, protein and glucose production, and energy balance. Monitoring these enzymes can reveal hidden health issues. Abnormal levels may result from dehydration, poor diet, medications, or genetic mutations. Improving liver, heart, and brain health requires better diet, exercise, hydration, and medication management. The rise in obesity and NAFLD, both linked to abnormal ALT/AST, underscores the importance of prevention to reduce risks of chronic diseases like heart attack, stroke, and dementia.
Source References and Supplemental Research:
1. Levinson M, Holbert J, Blackwell C, Wruble LD. Serum gamma-glutamyl transpeptidase: its specificity and clinical value. South Med J. 1979;72(7):837-841. doi:10.1097/00007611-197907000-00021. [PubMed]
2. Kasarala G, Tillmann HL. Standard liver tests. Clin Liver Dis (Hoboken). 2016;8(1):13-18. Published 2016 Jul 26. doi:10.1002/cld.562 [PubMed]
3. Klatskin G. Some observations on liver function tests. Yale.J Biol Med 1948;21(2):127‑43. [PubMed]
4. Kreider RB, Kalman DS, Antonio J, et al. International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. J Int Soc Sports Nutr. 2017;14:18. Published 2017 Jun 13. doi:10.1186/s12970-017-0173-z [PubMed][Cross Ref]
5. Oh RC, Hustead TR. Causes and evaluation of mildly elevated liver transaminase levels. Am Fam Physician.2011;84(9):1003‑8. [PubMed][Cross Ref]
6. Wu G. Amino acids: metabolism, functions, and nutrition. Amino Acids. 2009;37(1):1-17. doi:10.1007/s00726-009-0269-0 [Pubmed][Crossref]
7. de Koning TJ. Amino acid synthesis deficiencies. J Inherit Metab Dis. 2017;40(4):609-620. doi:10.1007/s10545-017-0063-1 [Pubmed][CrossRef]
8. Hohenester E, Jansonius JN. Crystalline mitochondrial aspartate aminotransferase exists in only two conformations. J Mol Biol. 1994;236(4):963-968.and RCSB PDB. [PubMed]
9. Wisniewska, M., Siponen, M.I., Arrowsmith, C.H., Berglund, H., Bountra, C., Collins, R., Edwards, A.M., Flodin, S., Flores, A., Graslund, S., Hammarstrom, M., Johansson, A., Johansson, I., Karlberg, T., Kotenyova, T., Kotzsch, A., Moche, M., Nielsen, T.K., Nordlund, P., Nyman, T., Persson, C., Roos, A.K., Schutz, P., Svensson, L., Thorsell, A.G., Tresaugues, L., Van Den Berg, S., Weigelt, J., Welin, M., Schuler, H., Structural Genomics Consortium (SGC) https://doi.org/10.2210/pdb3ihj/pdb and RCSB PDB.
10. Rui L. Energy metabolism in the liver. Compr Physiol. 2014;4(1):177-197. doi:10.1002/cphy.c130024 [PubMed][CrossRef]
11. Jakubowski H., Flatt P. Metabolic Fates of Amino Groups. LibreTexts Biology. https://bio.libretexts.org/Bookshelves/Biochemistry/Fundamentals_of_Biochemistry_%28Jakubowski_and_Flatt%29/02%3A_Unit_II-_Bioenergetics_and_Metabolism/18%3A_Nitrogen_-_Amino_Acid_Catabolism/18.02%3A_Metabolic_Fates_of_Amino_Groups
12. Cynober L. Metabolism of Dietary Glutamate in Adults. Ann Nutr Metab. 2018;73 Suppl 5:5-14. doi:10.1159/000494776 [PubMed][CrossRef]
13. Brosnan JT. Glutamate, at the interface between amino acid and carbohydrate metabolism. J Nutr. 2000;130(4S Suppl):988S-90S. doi:10.1093/jn/130.4.988S [PubMed][CrossRef]
14. Ito S. GABA and glycine in the developing brain. J Physiol Sci. 2016;66(5):375-379. doi:10.1007/s12576-016-0442-7 [PubMed][Cross Ref]
15. TJ Maher, BS Glaeser, RJ Wurtman. Diurnal variations in plasma concentrations of basic and neutral amino acids and in red cell concentrations of aspartate and glutamate: effects of dietary protein intake. Am J Clin Nutr. 1984;39(5):722–9. doi:10.1093/ajcn/39.5.722 [PubMed]
16. Loï C, Cynober L. Glutamate: A Safe Nutrient, Not Just a Simple Additive. Ann Nutr Metab. 2022;78(3):133-146. doi:10.1159/000522482 [PubMed]
17. Olsen RW, DeLorey TM. GABA Receptor Physiology and Pharmacology. In: Siegel GJ, Agranoff BW, Albers RW, et al., editors. Basic Neurochemistry: Molecular, Cellular and Medical Aspects. 6th edition. Philadelphia: Lippincott-Raven; 1999. https://www.ncbi.nlm.nih.gov/books/NBK28090/
18. D’Aniello A. D-Aspartic acid: An endogenous amino acid with an important neuroendocrine role. Brain Res. Rev. 2007;53(2):215–234. doi: 10.1016/j.brainresrev.2006.08.005. [PubMed][CrossRef]
19. D’Aniello A, Luongo L, Romano R, et al. d-Aspartic acid ameliorates painful and neuropsychiatric changes and reduces β-amyloid Aβ1-42 peptide in a long lasting model of neuropathic pain. Neurosci Lett. 2017;651:151-158. doi:10.1016/j.neulet.2017.04.041 [PubMed] [CrossRef]
20. Nelson D, Cox M. Chapter 18: Amino Acid Oxidation and the Production of Urea. In: Lehninger Principles of Biochemistry. 4th ed. 2005: 684-685
21. Ishiguro M, Takio K, Suzuki M, Oyama R, Matsuzawa T, Titani K. Complete amino acid sequence of human liver cytosolic alanine aminotransferase (GPT) determined by a combination of conventional and mass spectral methods. Biochemistry. 1991;30(43):10451-10457. doi:10.1021/bi00107a013 [PubMed]
22. Coss CC, Bauler M, Narayanan R, Miller DD, Dalton JT. Alanine aminotransferase regulation by androgens in non-hepatic tissues. Pharm Res. 2012;29(4):1046-1056. doi:10.1007/s11095-011-0649-5 [PubMed][CrossRef]
23. Sherman KE. Alanine aminotransferase in clinical practice. A review. Arch Intern Med. 1991;151(2):260-265. [PubMed][CrossRef]
24. Senior JR. Alanine aminotransferase: a clinical and regulatory tool for detecting liver injury-past, present, and future. Clin Pharmacol Ther. 2012;92(3):332-339. doi:10.1038/clpt.2012.108 [PubMed][CrossRef]
25. O’Shea RS, Dasarathy S, McCullough AJ; Practice Guideline Committee of the American Association for the Study of Liver Diseases; Practice Parameters Committee of the American College of Gastroenterology. Alcoholic liver disease. Hepatology. 2010;51(1):307-28. doi:10.1002/hep.23258 [PubMed]
26. Lee J.H., Friso S., Choi S.W. Epigenetic mechanisms underlying the link between non-alcoholic fatty liver diseases and nutrition. Nutrients. 2014;6:3303–3325. doi: 10.3390/nu6083303. [PubMed]
27. Clark JM, Brancati FL, Diehl AM. The prevalence and etiology of elevated aminotransferase levels in the United States. Am J Gastroenterol. 2003;98(5):960-967. doi:10.1111/j.1572-0241.2003.07486.x [PubMed] [CrossRef]
28. Montonen J, Boeing H, Schleicher E, Fritsche A, Pischon T. Association of changes in body mass index during earlier adulthood and later adulthood with circulating obesity biomarker concentrations in middle-aged men and women. Diabetologia. 2011;54(7):1676–1683. doi: 10.1007/s00125-011-2124-6. [PubMed] [CrossRef]
29. Robinson D, Whitehead TP. Effect of body mass and other factors on serum liver enzyme levels in men attending for well population screening. Ann Clin Biochem. 1989;26 ( Pt 5):393-400. doi:10.1177/000456328902600503 [PubMed][CrossRef]
30. Usui C, Asaka M, Kawano H, et al. Visceral fat is a strong predictor of insulin resistance regardless of cardiorespiratory fitness in non-diabetic people. J Nutr Sci Vitaminol (Tokyo). 2010;56(2):109-116. doi:10.3177/jnsv.56.109 [PubMed][CrossRef]
31. Ko YH, Wong TC, Hsu YY, Kuo KL, Yang SH. The Correlation Between Body Fat, Visceral Fat, and Nonalcoholic Fatty Liver Disease. Metab Syndr Relat Disord. 2017;15(6):304-311. doi:10.1089/met.2017.0001 [PubMed]
32. Fraser A, Longnecker MP, Lawlor DA. Prevalence of elevated alanine aminotransferase among US adolescents and associated factors: NHANES 1999-2004. Gastroenterology. 2007;133(6):1814-1820. doi:10.1053/j.gastro.2007.08.077 [PubMed][CrossRef]
33. Ruhl CE, Everhart JE. Determinants of the association of overweight with elevated serum alanine aminotransferase activity in the United States. Gastroenterology. 2003;124(1):71-79. doi:10.1053/gast.2003.50004 [PubMed][CrossRef]
34. Trilk JL, Ortaglia A, Blair SN, Bottai M, Church TS, Pate RR. Cardiorespiratory fitness, waist circumference, and alanine aminotransferase in youth. Med Sci Sports Exerc. 2013;45(4):722-727. doi:10.1249/MSS.0b013e31827aa875 [PubMed]
35. Stranges S, Dorn JM, Muti P, et al. Body fat distribution, relative weight, and liver enzyme levels: a population-based study. Hepatology. 2004;39(3):754-763. doi:10.1002/hep.20149 [PubMed]
36. Song HR, Yun KE, Park HS. Relation between alanine aminotransferase concentrations and visceral fat accumulation among nondiabetic overweight Korean women. Am J Clin Nutr. 2008;88(1):16-21. doi:10.1093/ajcn/88.1.16 [PubMed][CrossRef]
37. G Arancibia, H García, F Jaime, R Bancalari, PR Harris. Association of metabolic syndrome markers with abnormal alanine aminotransferase levels in healthy children. Rev Med Chil. 2012;140(7):896-901. doi: 10.4067/S0034-98872012000700010.[PubMed][CrossRef]
38. Ehrlich S, Burghardt R, Weiss D, et al. Glial and neuronal damage markers in patients with anorexia nervosa. J Neural Transm (Vienna). 2008;115(6):921-927. doi:10.1007/s00702-008-0033-8 [PubMed] [CrossRef]
39. Güngör B, Cağlayan K, Polat C, Seren D, Erzurumlu K, Malazgirt Z. The predictivity of serum biochemical markers in acute biliary pancreatitis. ISRN Gastroenterol. 2011;2011:279607. doi:10.5402/2011/279607 [PubMed]
40. King LG, Seelig CB, Ranney JE. The lipase to amylase ratio in acute pancreatitis. Am J Gastroenterol. 1995;90(1):67-69. [PubMed]
41. Kalloo AN, Kantsevoy SV. Gallstones and biliary disease. Prim Care. 2001;28(3):591-vii. doi:10.1016/s0095-4543(05)70055-5 [PubMed]
42. Anderson K, Brown LA, Daniel P, Connor SJ. Alanine transaminase rather than abdominal ultrasound alone is an important investigation to justify cholecystectomy in patients presenting with acute pancreatitis. HPB (Oxford). 2010;12(5):342-347. doi:10.1111/j.1477-2574.2010.00173.x [PubMed][CrossRef]
43. Singh A, Koritala T, Jialal I. Unconjugated Hyperbilirubinemia.. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. https://www.ncbi.nlm.nih.gov/books/NBK549796
44. Good WV, Hou C. Visuocortical bilirubin-induced neurological dysfunction. Semin Fetal Neonatal Med. 2015 Feb;20(1):37-41. [PubMed]
45. Olds C, Oghalai JS. Audiologic impairment associated with bilirubin-induced neurologic damage. Semin Fetal Neonatal Med. 2015 Feb;20(1):42-46. [PMC free article] [PubMed]
46. Rose J, Vassar R. Movement disorders due to bilirubin toxicity. Semin Fetal Neonatal Med. 2015 Feb;20(1):20-25. [PMC free article] [PubMed]
47. Wusthoff CJ, Loe IM. Impact of bilirubin-induced neurologic dysfunction on neurodevelopmental outcomes. Semin Fetal Neonatal Med. 2015 Feb;20(1):52-57. [PMC free article] [PubMed]
48. Rehm J. The risks associated with alcohol use and alcoholism. Alcohol Res Health. 2011;34(2):135-143. [PubMed]
49. Boffetta P, Hashibe M. Alcohol and cancer. Lancet Oncol. 2006;7(2):149-156. doi:10.1016/S1470-2045(06)70577-0 [PubMed][CrossRef]
50. Seitz HK, Becker P. Alcohol metabolism and cancer risk. Alcohol Res Health. 2007;30(1):38-47.[PubMed] [CrossRef]
51. Lachenmeier DW, Kanteres F, Rehm J. Carcinogenicity of acetaldehyde in alcoholic beverages: risk assessment outside ethanol metabolism. Addiction. 2009;104(4):533-550. doi:10.1111/j.1360-0443.2009.02516.x [PubMed] [CrossRef]
52. Fuentealba IC, Aburto EM. Animal models of copper-associated liver disease. Comp Hepatol. 2003;2(1):5. Published 2003 Apr 3. doi:10.1186/1476-5926-2-5 [PubMed][Crossref]
53. Harvard T. H. Chan School of Public Health. Copper. The Nutrition Source. March 2023.https://nutritionsource.hsph.harvard.edu/copper/
54. Collins JF, Klevay LM. Copper. Adv Nutr. 2011;2(6):520-522. doi:10.3945/an.111.001222 [PubMed]
55. Mason KE. A conspectus of research on copper metabolism and requirements of man. J Nutr. 1979;109(11):1979-2066. doi:10.1093/jn/109.11.1979 [CrossRef]
56. Oe S, Miyagawa K, Honma Y, Harada M. Copper induces hepatocyte injury due to the endoplasmic reticulum stress in cultured cells and patients with Wilson disease. Exp Cell Res. 2016;347(1):192-200. doi:10.1016/j.yexcr.2016.08.003 [PubMed] [Crossref]
57. Royer A, Sharman T. Copper Toxicity. [Updated 2023 Mar 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557456/
58. Sturniolo GC, Mestriner C, Irato P, Albergoni V, Longo G, D’Incà R. Zinc therapy increases duodenal concentrations of metallothionein and iron in Wilson’s disease patients. Am J Gastroenterol. 1999;94(2):334-338. doi:10.1111/j.1572-0241.1999.851_w.x [PubMed] [CrossRef]
59. Gamakaranage CS, Rodrigo C, Weerasinghe S, Gnanathasan A, Puvanaraj V, Fernando H. Complications and management of acute copper sulphate poisoning; a case discussion. J Occup Med Toxicol. 2011;6(1):34. Published 2011 Dec 19. doi:10.1186/1745-6673-6-34 [PubMed]
60. Subbiah V, West HJ. Jaundice (Hyperbilirubinemia) in Cancer. JAMA Oncol. 2016;2(8):1103. doi:10.1001/jamaoncol.2016.1236 [PubMed] [Crossref]
61. Paik, James M. Golabi, Pegah. Biswas, Rakesh. Alqahtani, Saleh. Venkatesan, Chapy. Younossi, Zobair M. Nonalcoholic Fatty Liver Disease and Alcoholic Liver Disease are Major Drivers of Liver Mortality in the United States. Hepatology Communications 4(6):p 890-903, June 2020. | DOI: 10.1002/hep4.1510 [Crossref]
62. Ioannou, George N. Boyko, Edward J. Lee, Sum P. The Prevalence and Predictors of Elevated Serum Aminotransferase Activity in the United States in 1999–2002. American Journal of Gastroenterology 101(1):p 76-82, January 2006. [Crossref]
63. Younossi, Zobair M. Koenig, Aaron B. Abdelatif, Dinan. Fazel, Yousef. Henry, Linda. Wymer, Mark. Global epidemiology of nonalcoholic fatty liver disease—Meta‐analytic assessment of prevalence, incidence, and outcomes. Hepatology 64(1):p 73-84, July 2016. | DOI: 10.1002/hep.28431 [CrossRef]
64. Huang, J., Gao, T., Zhang, H. et al. Association of obesity profiles and metabolic health status with liver injury among US adult population in NHANES 1999–2016. Sci Rep 13, 15958 (2023). https://doi.org/10.1038/s41598-023-43028-7 [CrossRef]
65. Cotter TG, Rinella M. Nonalcoholic Fatty Liver Disease 2020: The State of the Disease. Gastroenterology. 2020;158(7):1851-1864. doi:10.1053/j.gastro.2020.01.052 [PubMed][Crossref]
66. Ramsay DJ. Homeostatic control of water balance. In: Arnaud MJ, editor. Hydration Throughout Life. Montrouge: John Libbey Eurotext; 1998. pp. 9–18.
67. Bunn HF. Hemoglobin I. Structure and function. In: Beck WS, Hematology. Cambridge, MA: MIT Press, 1981;129.
68. Hom J, Dulmovits BM, Mohandas N, Blanc L. The erythroblastic island as an emerging paradigm in the anemia of inflammation. Immunol Res. 2015;63(1-3):75-89. doi:10.1007/s12026-015-8697-2 [PubMed]
69. Chung J, Chen C, Paw BH. Heme metabolism and erythropoiesis. Curr Opin Hematol. 2012;19(3):156-162. doi:10.1097/MOH.0b013e328351c48b [PubMed][CrossRef]
70. Weiss G. Iron metabolism in the anemia of chronic disease. Biochim Biophys Acta. 2009;1790(7):682-693. doi:10.1016/j.bbagen.2008.08.006 [PubMed][CrossRef]
71. Weiss G, Goodnough LT. Anemia of chronic disease. N Engl J Med. 2005;352(10):1011-1023. doi:10.1056/NEJMra041809 [PubMed][CrossRef]
72. Wallerstein RO. Laboratory evaluation of anemia. West J Med. 1987;146:443.
73. Billett H. Chapter 151: Hemoglobin and Hematocrit. Clinical Methods: The History, Physical and Laboratory Examinations. 3rd Edition. Boston: Butterworths; 1990.
74. Ravasi G, Pelucchi S, Greni F, et al. Circulating factors are involved in hypoxia-induced hepcidin suppression. Blood Cells Mol Dis. 2014;53(4):204-210. doi:10.1016/j.bcmd.2014.06.006 [PubMed][CrossRef]
75. Nemeth E, Valore EV, Territo M, Schiller G, Lichtenstein A, Ganz T. Hepcidin, a putative mediator of anemia of inflammation, is a type II acute-phase protein. Blood. 2003;101(7):2461-2463. doi:10.1182/blood-2002-10-3235 [PubMed][CrossRef]
76. EA Galushko. The clinical significance of hepcidin detection in patients with anemia and rheumatoid arthritis (in Russian) Klin Med (Mosk) 2014;92:21–27. [PubMed]
77. Scalise V, Balia C, Cianchetti S, et al. Non enzymatic upregulation of tissue factor expression by gamma-glutamyl transferase in human peripheral blood mononuclear cells. Thromb J. 2016;14:45. Published 2016 Nov 4. doi:10.1186/s12959-016-0119-8[PubMed]
78. Wessling-Resnick M. Iron. In: Ross AC, Caballero B, Cousins RJ, Tucker KL, Ziegler RG, eds. Modern Nutrition in Health and Disease. 11th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2014:176-88. [CrossRef]
79. Aggett PJ. Iron. In: Erdman JW, Macdonald IA, Zeisel SH, eds. Present Knowledge in Nutrition. 10th ed. Washington, DC: Wiley-Blackwell; 2012:506-20.
80. Drakesmith H, Prentice AM. Hepcidin and the Iron-Infection Axis. Science 2012;338:768-72. [PubMed abstract]
81. Halliwell B., Gutteridge J.M. Role of free radicals and catalytic metal irons in human disease: An overview. Methods Enzymol. 1990;186:1–85. doi: 10.1016/0076-6879(90)86093-B. [PubMed] [CrossRef] [Google Scholar]
82. Tiedge M., Lortz S., Drinkgern J., Lenzen S. Relation between antioxidant enzyme gene expression and antioxidative defense status of insulin-producing cells. Diabetes. 1997;46:1733–1742. doi: 10.2337/diab.46.11.1733. [PubMed] [CrossRef] [Google Scholar]
83. Swaminathan S., Fonseca V.A., Alam M.G., Shah S.V. The role of iron in diabetes and its complications. Diabetes Care. 2007;30:1926–1933. doi: 10.2337/dc06-2625. [PubMed] [CrossRef] [Google Scholar]
84. Wilson J.G., Lindquist J.H., Grambow S.C., Crook E.D., Maher J.F. Potential role of increased iron stores in diabetes. Am. J. Med. Sci. 2003;325:332–339. doi: 10.1097/00000441-200306000-00004. [PubMed] [CrossRef] [Google Scholar]
85. De Valk B., Marx J.J. Iron, Atherosclerosis, and ischemic heart disease. Arch. Intern. Med. 1999;159:1542–1548. doi: 10.1001/archinte.159.14.1542. [PubMed] [CrossRef] [Google Scholar]
86. Tappel A. Heme of consumed red meat can act as a catalyst of oxidative damage and could initiate colon, breast and prostate cancers, heart disease and other diseases. Med. Hypotheses. 2007;68:562–564. doi: 10.1016/j.mehy.2006.08.025. [PubMed] [CrossRef] [Google Scholar]
87. Andrews N.C. Disorders of iron metabolism. N. Engl. J. Med. 1999;341:1986–1995. doi: 10.1056/NEJM199912233412607. [PubMed] [CrossRef] [Google Scholar]
88. Dludla P.V., Joubert E., Muller C.J.F., Louw J., Johnson R. Hyperglycemia-induced oxidative stress and heart disease-cardioprotective effects of rooibos flavonoids and phenylpyruvic acid-2-O-beta-D-glucoside. Nutr. Metab. 2017;14:45. doi: 10.1186/s12986-017-0200-8. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
89. Han C.Y. Roles of Reactive Oxygen Species on Insulin Resistance in Adipose Tissue. Diabetes Metab. J. 2016;40:272–279. doi: 10.4093/dmj.2016.40.4.272. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
90. Stocker R, Yamamoto Y, McDonagh AF, Glazer AN, Ames BN. Bilirubin is an antioxidant of possible physiological importance. Science. 1987;235(4792):1043-1046. doi:10.1126/science.3029864 [PubMed]
91. Furukawa S., Fujita T., Shimabukuro M., Iwaki M., Yamada Y., Nakajima Y., Nakayama O., Makishima M., Matsuda M., Shimomura I. Increased oxidative stress in obesity and its impact on metabolic syndrome. J. Clin. Investig. 2004;114:1752–1761. doi: 10.1172/JCI21625. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
92. Sies H. Oxidative stress: A concept in redox biology and medicine. Redox Biol. 2015;4:180–183. doi: 10.1016/j.redox.2015.01.002. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
93. Liao Y.F., Zhu W., Li D.P., Zhu X. Heme oxygenase-1 and gut ischemia/reperfusion injury: A short review. World J. Gastroenterol. 2013;19:3555–3561. doi: 10.3748/wjg.v19.i23.3555. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
94. Schipper H.M. Heme oxygenase-1 in Alzheimer disease: A tribute to moussa youdim. J. Neural. Transm. 2011;118:381–387. doi: 10.1007/s00702-010-0436-1. [PubMed] [CrossRef] [Google Scholar]
95. Origassa C.S., Camara N.O. Cytoprotective role of heme oxygenase-1 and heme degradation derived end products in liver injury. World J. Hepatol. 2013;5:541–549. [PMC free article] [PubMed] [Google Scholar]
96. Zhang L., Sessoms R. Heme Biology. World Scientific Publishing Company; Singapore: 2011. Heme Biosynthesis and Degradation: What Happens When It Goes Haywire? pp. 7–31. [Google Scholar]
97. Dawson PA, Lan T, Rao A. Bile acid transporters. J Lipid Res. 2009;50(12):2340–2357. [PMC free article] [PubMed] [Google Scholar]
98. Stieger B. Role of the bile salt export pump, BSEP, in acquired forms of cholestasis. Drug Metab Rev. 2010;42(3):437–445. [PubMed] [Google Scholar]
99. Georgiev P, Jochum W, Heinrich S, et al. Characterization of time-related changes after experimental bile duct ligation. Br J Surg. 2008;95(5):646–656. [PubMed] [Google Scholar]
100. Miyoshi H, Rust C, Roberts PJ, Burgart LJ, Gores GJ. Hepatocyte apoptosis after bile duct ligation in the mouse involves Fas. Gastroenterology. 1999;117(3):669–677. [PubMed] [Google Scholar]
101. Badminton M.N., Elder G.H. Molecular mechanisms of dominant expression in porphyria. J. Inherit Metab. Dis. 2005;28:277–286. doi: 10.1007/s10545-005-8050-3. [PubMed] [CrossRef] [Google Scholar]
102. Rangan C, Barceloux DG. Food additives and sensitivities. Dis Mon. 2009;55(5):292-311. doi:10.1016/j.disamonth.2009.01.004 [PubMed][Crossref]
103. Tennant DR. Review of Glutamate Intake from Both Food Additive and Non-Additive Sources in the European Union. Ann Nutr Metab. 2018;73 Suppl 5:21-28. doi:10.1159/000494778 [PubMed] [Crossref]
104. Tomé D. The Roles of Dietary Glutamate in the Intestine. Ann Nutr Metab. 2018;73 Suppl 5:15-20. doi:10.1159/000494777 [PubMed][Crossref]
105. Zhang Y, Venkitasamy C, Pan Z, Liu W, Zhao L. Novel Umami Ingredients: Umami Peptides and Their Taste. J Food Sci. 2017;82(1):16-23. doi:10.1111/1750-3841.13576 [PubMed][Crossref]
106 Forde BG, Lea PJ. Glutamate in plants: metabolism, regulation, and signaling. J Exp Bot. 2007;58(9):2339-2358. doi:10.1093/jxb/erm121 [PubMed][Crossref]
107. Jander G, Joshi V. Recent progress in deciphering the biosynthesis of aspartate-derived amino acids in plants. Mol Plant. 2010;3(1):54-65. doi:10.1093/mp/ssp104 [PubMed][Crossref]
108. Zhang H, Tsao R. Dietary polyphenols, oxidative stress and antioxidant and anti-inflammatory effects. Curr Opin Food Sci. (2016) 8:33–42. 10.1016/j.cofs.2016.02.002 [CrossRef] [Google Scholar]
109. Hurrell R, Egli I. Iron bioavailability and dietary reference values. Am J Clin Nutr. (2010) 91:1461S−7S. 10.3945/ajcn.2010.28674F [PubMed] [CrossRef] [Google Scholar]
110. Kwok RH. Chinese-restaurant syndrome. N Engl J Med. 1968;278(14):796. doi:10.1056/nejm196804042781419 [PubMed][Crossref]
111. Yang WH, Drouin MA, Herbert M, Mao Y, Karsh J. The monosodium glutamate symptom complex: assessment in a double-blind, placebo-controlled, randomized study. J Allergy Clin Immunol. 1997;99(6 Pt 1):757-762. doi:10.1016/s0091-6749(97)80008-5 [PubMed]
112. Rowley NM, Madsen KK, Schousboe A, Steve White H. Glutamate and GABA synthesis, release, transport and metabolism as targets for seizure control. Neurochem Int. 2012;61(4):546-558. doi:10.1016/j.neuint.2012.02.013 [PubMed] [Crossref]
113. Südhof TC. Neurotransmitter release: the last millisecond in the life of a synaptic vesicle. Neuron. 2013;80(3):675-690. doi:10.1016/j.neuron.2013.10.022 [PubMed]
114. Lewerenz J, Maher P. Chronic Glutamate Toxicity in Neurodegenerative Diseases-What is the Evidence?. Front Neurosci. 2015;9:469. Published 2015 Dec 16. doi:10.3389/fnins.2015.00469 [PubMed] [Crossref]
115. Tzschentke TM, Schmidt WJ. Glutamatergic mechanisms in addiction. Mol Psychiatry. 2003;8(4):373-382. doi:10.1038/sj.mp.4001269 [PubMed] [Crossref]
116. Office of dietary supplements – Iron. NIH Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/Iron-HealthProfessional/
117. Institute of Medicine. Food and Nutrition Board. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc : a Report of the Panel on Micronutrients. Washington, DC: National Academy Press; 2001. [CrossRef]
118. Murray-Kolbe LE, Beard J. Iron. In: Coates PM, Betz JM, Blackman MR, et al., eds. Encyclopedia of Dietary Supplements. 2nd ed. London and New York: Informa Healthcare; 2010:432-8.
119. Rajpathak S., Ma J., Manson J., Willett W.C., Hu F.B. Iron intake and the risk of type 2 diabetes in women: A Prospective Cohort Study. Diabetes Care. 2006;29:1370–1376. doi: 10.2337/dc06-0119. [PubMed] [CrossRef] [Google Scholar]
120. Schwartz S, Ellefson M. Quantitative fecal recovery of ingested hemoglobin-heme in blood: comparisons by HemoQuant assay with ingested meat and fish. Gastroenterology. 1985;89(1):19-26. doi:10.1016/0016-5085(85)90740-1[PubMed]
121. Han O. Molecular mechanism of intestinal iron absorption. Metallomics. 2011;3(2):103-109. doi:10.1039/c0mt00043d [PubMed][Crossref]
122. Krishnamurthy P., Xie T., Schuetz J.D. The role of transporters in cellular heme and porphyrin homeostasis. Pharmacol. Ther. 2007;114:345–358. [PubMed] [Google Scholar]
123. Beutler E., Bothwell T.H., Charlton R.W., Motulsky A.G. Hereditary Hemochromatosis. The McGraw-Hill Companies; New York, NY, USA: 2006. [Google Scholar]
124. West A.R., Oates P.S. Mechanisms of heme iron absorption: Current questions and controversies. World J. Gastroenterol. 2008;14:4101–4110. doi: 10.3748/wjg.14.4101. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
125. Hooda J, Shah A, Zhang L. Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients. 2014;6(3):1080-1102. Published 2014 Mar 13. doi:10.3390/nu6031080 [PubMed]
126. Song Y, Liu J, Zhao K, Gao L, Zhao J. Cholesterol-induced toxicity: An integrated view of the role of cholesterol in multiple diseases. Cell Metab. 2021;33(10):1911-1925. doi:10.1016/j.cmet.2021.09.001 [PubMed][Crossref]
127. Hooda J., Cadinu D., Alam M.M., Shah A., Cao T.M., Sullivan L.A., Brekken R., Zhang L. Enhanced heme function and mitochondrial respiration promote the progression of lung cancer cells. PLoS One. 2013;8:e63402. [PMC free article] [PubMed] [Google Scholar]
128. Sritharan M (July 2006). “Iron and bacterial virulence”. Indian J Med Microbiol. 24 (3): 163–4. doi:10.1016/S0255-0857(21)02343-4. PMID 16912433. [PubMed]
129. Jiang R., Ma J., Ascherio A., Stampfer M.J., Willett W.C., Hu F.B. Dietary iron intake and blood donations in relation to risk of type 2 diabetes in men: A prospective cohort study. Am. J. Clin. Nutr. 2004;79:70–75. [PubMed] [Google Scholar]
130. Zhao Z., Li S., Liu G., Yan F., Ma X., Huang Z., Tian H. Body iron stores and heme-iron intake in relation to risk of type 2 diabetes: A systematic review and meta-analysis. PLoS One. 2012;7:e41641. [PMC free article] [PubMed] [Google Scholar]
131. Jehn M.L., Guallar E., Clark J.M., Couper D., Duncan B.B., Ballantyne C.M., Hoogeveen R.C., Harris Z.L., Pankow J.S. A prospective study of plasma ferritin level and incident diabetes: The Atherosclerosis Risk in Communities (ARIC) Study. Am. J. Epidemiol. 2007;165:1047–1054. doi: 10.1093/aje/kwk093. [PubMed] [CrossRef] [Google Scholar]
132. Qiu C., Zhang C., Gelaye B., Enquobahrie D.A., Frederick I.O., Williams M.A. Gestational diabetes mellitus in relation to maternal dietary heme iron and nonheme iron intake. Diabetes Care. 2011;34:1564–1569. doi: 10.2337/dc11-0135. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
133. Ascherio A., Hennekens C.H., Buring J.E., Master C., Stampfer M.J., Willett W.C. Trans-fatty acids intake and risk of myocardial infarction. Circulation. 1994;89:94–101. doi: 10.1161/01.CIR.89.1.94. [PubMed] [CrossRef] [Google Scholar]
134. Snowdon D.A., Phillips R.L., Fraser G.E. Meat consumption and fatal ischemic heart disease. Prev. Med. 1984;13:490–500. doi: 10.1016/0091-7435(84)90017-3. [PubMed] [CrossRef] [Google Scholar]
135. Kleinbongard P., Dejam A., Lauer T., Jax T., Kerber S., Gharini P., Balzer J., Zotz R.B., Scharf R.E., Willers R., et al. Plasma nitrite concentrations reflect the degree of endothelial dysfunction in humans. Free Radic. Biol. Med. 2006;40:295–302. doi: 10.1016/j.freeradbiomed.2005.08.025. [PubMed] [CrossRef] [Google Scholar]
136. Mannisto S., Kontto J., Kataja-Tuomola M., Albanes D., Virtamo J. High processed meat consumption is a risk factor of type 2 diabetes in the α-tocopherol, β-carotene cancer prevention study. Br. J. Nutr. 2010;103:1817–1822. doi: 10.1017/S0007114510000073. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
137. Vannella L, Aloe Spiriti MA, Cozza G, Tardella L, Monarca B, Cuteri A, et al. Benefit of concomitant gastrointestinal and gynecological evaluation in premenopausal women with iron deficiency anemia. Aliment Pharmacol Ther 2008;28:422-30. [PubMed abstract]
138. Cory H, Passarelli S, Szeto J, Tamez M, Mattei J. The Role of Polyphenols in Human Health and Food Systems: A Mini-Review. Front Nutr. 2018;5:87. Published 2018 Sep 21. doi:10.3389/fnut.2018.00087 [PubMed]
139. Rutzke CJ, Glahn RP, Rutzke MA, et al. Bioavailability of iron from spinach using an in vitro/human Caco-2 cell bioassay model. Habitation (Elmsford). 2004;10(1):7-14. doi:10.3727/154296604774808900[PubMed abstract]
140. Gillooly M, Bothwell TH, Torrance JD, et al. The effects of organic acids, phytates and polyphenols on the absorption of iron from vegetables. Br J Nutr. 1983;49(3):331-342. doi:10.1079/bjn19830042 [PubMed][CrossRef]
141. Consoli A, Nurjhan N, Capani F, Gerich J. Predominant role of gluconeogenesis in increased hepatic glucose production in NIDDM. Diabetes. 1989;38:550–557. [PubMed] [Google Scholar]
142. Magnusson I, Rothman DL, Katz LD, Shulman RG, Shulman GI. Increased rate of gluconeogenesis in type II diabetes mellitus. A 13C nuclear magnetic resonance study. J Clin Invest. 1992;90:1323–1327. [PMC free article] [PubMed] [Google Scholar]
143. Meyer C, Stumvoll M, Nadkarni V, Dostou J, Mitrakou A, Gerich J. Abnormal renal and hepatic glucose metabolism in type 2 diabetes mellitus. J Clin Invest. 1998;102:619–624. [PMC free article] [PubMed] [Google Scholar]
144. McGill MR, Jaeschke H. Metabolism and disposition of acetaminophen: recent advances in relation to hepatotoxicity and diagnosis. Pharm Res. 2013;30(9):2174-2187. doi:10.1007/s11095-013-1007-6 [PubMed]
145. Ashar U, Desai D, Bhaduri A. Flutamide-induced hepatotoxicity with possible potentiation by simvastatin. J Assoc Physicians India. 2003;51:75-77. [PubMed]
146. Yin LK, Tong KS. Elevated Alt and Ast in an Asymptomatic Person: What the primary care doctor should do?. Malays Fam Physician. 2009;4(2-3):98-99. Published 2009 Aug 31.[PubMed][CrossRef]
147. Whitcomb DC, Block GD. Association of acetaminophen hepatotoxicity with fasting and ethanol use. JAMA. 1994;272(23):1845-1850. doi:10.1001/jama.1994.03520230055038 [PubMed] [Crossref]
148. Reuben A, Koch DG, Lee WM; Acute Liver Failure Study Group. Drug-induced acute liver failure: results of a U.S. multicenter, prospective study. Hepatology. 2010;52(6):2065-2076. doi:10.1002/hep.23937 [PubMed]
149. Hoy SM, Lyseng-Williamson KA. Intravenous busulfan: in the conditioning treatment of pediatric patients prior to hematopoietic stem cell transplantation. Paediatr Drugs. 2007;9(4):271-278. doi:10.2165/00148581-200709040-00008 [PubMed][CrossRef]
150. Geubel AP, De Galocsy C, Alves N, Rahier J, Dive C. Liver damage caused by therapeutic vitamin A administration: estimate of dose-related toxicity in 41 cases. Gastroenterology. 1991;100(6):1701-1709. doi:10.1016/0016-5085(91)90672-8 [PubMed]
151. Guollo F, Narciso-Schiavon JL, Barotto AM, Zannin M, Schiavon LL. Significance of alanine aminotransferase levels in patients admitted for cocaine intoxication. J Clin Gastroenterol. 2015;49(3):250-255. doi:10.1097/MCG.0000000000000056 [PubMed] [Crossref]
152. Kuo CJ, Tsai SY, Liao YT, et al. Elevated aspartate and alanine aminotransferase levels and natural death among patients with methamphetamine dependence [published correction appears in PLoS One. 2012;7(1). doi:10.1371/annotation/3bca7672-2fca-4a7e-942d-cc1b4aaa7b60] [published correction appears in PLoS One. 2012;7(1). doi:10.1371/annotation/85803bd9-3be6-4450-b70f-cd4104b87817]. PLoS One. 2012;7(1):e29325. doi:10.1371/journal.pone.0029325 [PubMed]
153. Lee WM. Drug-induced hepatotoxicity. N Engl J Med. 2003;349(5):474-485. doi:10.1056/NEJMra021844 [PubMed][CrossRef]
154. Larrey D, Pageaux GP. Drug-induced acute liver failure. Eur J Gastroenterol Hepatol. 2005;17(2):141-143. doi:10.1097/00042737-200502000-00002 [PubMed][Crossref]
155.Fontana RJ, Hayashi PH, Gu J, et al. Idiosyncratic drug-induced liver injury is associated with substantial morbidity and mortality within 6 months from onset. Gastroenterology. 2014;147(1):96-108.e4. doi:10.1053/j.gastro.2014.03.045.[PubMed][CrossRef]
156. McGill MR, Sharpe MR, Williams CD, Taha M, Curry SC, Jaeschke H. The mechanism underlying acetaminophen-induced hepatotoxicity in humans and mice involves mitochondrial damage and nuclear DNA fragmentation. J Clin Invest. 2012;122(4):1574-1583. doi:10.1172/JCI59755. [PubMed][CrossRef]
157. Yuan L, Kaplowitz N. Mechanisms of drug-induced liver injury. Clin Liver Dis. 2013;17(4):507-vii. doi:10.1016/j.cld.2013.07.002 [PubMed][CrossRef]
158. Russmann S, Jetter A, Kullak-Ublick GA. Pharmacogenetics of drug-induced liver injury. Hepatology. 2010;52(2):748-761. doi:10.1002/hep.23720[PubMed]
159. Devarbhavi H, Raj S, Aradya VH, et al. Drug-induced liver injury associated with Stevens-Johnson syndrome/toxic epidermal necrolysis: Patient characteristics, causes, and outcome in 36 cases. Hepatology. 2016;63(3):993-999. doi:10.1002/hep.28270 [PubMed][CrossRef]
160. Razavi Zade M, Telkabadi MH, Bahmani F, Salehi B, Farshbaf S, Asemi Z. The effects of DASH diet on weight loss and metabolic status in adults with non-alcoholic fatty liver disease: a randomized clinical trial. Liver Int. 2016;36(4):563-571. doi:10.1111/liv.12990 [PubMed][Crossref]
161.Azadbakht L, Surkan PJ, Esmaillzadeh A, Willett WC. The Dietary Approaches to Stop Hypertension eating plan affects C-reactive protein, coagulation abnormalities, and hepatic function tests among type 2 diabetic patients. J Nutr. 2011;141(6):1083-1088. doi:10.3945/jn.110.136739 [PubMed][CrossRef]
162. Alferink LJM, Erler NS, de Knegt RJ, et al. Adherence to a plant-based, high-fibre dietary pattern is related to regression of non-alcoholic fatty liver disease in an elderly population. Eur J Epidemiol. 2020;35(11):1069-1085. doi:10.1007/s10654-020-00627-2 [PubMed][Crossref]
163. De Chiara F, Ureta Checcllo C, Ramón Azcón J. High Protein Diet and Metabolic Plasticity in Non-Alcoholic Fatty Liver Disease: Myths and Truths. Nutrients. 2019;11(12):2985. Published 2019 Dec 6. doi:10.3390/nu11122985 [PubMed][Crossref]
164. Fakhoury-Sayegh N, Younes H, Heraoui GNHA, Sayegh R. Nutritional Profile and Dietary Patterns of Lebanese Non-Alcoholic Fatty Liver Disease Patients: A Case-Control Study. Nutrients. 2017;9(11):1245. Published 2017 Nov 14. doi:10.3390/nu9111245 [PubMed] [Crossref]
165. Maroto-Sánchez B, Lopez-Torres O, Valtueña J, et al. Rehydration during exercise prevents the increase of homocysteine concentrations. Amino Acids. 2019;51(2):193-204. doi:10.1007/s00726-018-2655-y [PubMed][CrossRef]
166. Kennedy M, Crozier S. How much water you’re actually supposed to drink each day — and why 8 cups isn’t right for everyone. Business Insiders: Reviews. December 14, 2021. https://www.businessinsider.com/guides/health/diet-nutrition/how-much-water-should-i-drink
167. Bari MA, Mahmood, Alobaidi MA, Ansari HA, et al. Effects of an aerobic training program on liver functions in male athletes: a randomized controlled trial. Sci Rep. 2023;13(1):9427. Published 2023 Jun 9. doi:10.1038/s41598-023-36361-4 [PubMed][CrossRef]
168. Deminice R, Ribeiro DF, Frajacomo FT. The Effects of Acute Exercise and Exercise Training on Plasma Homocysteine: A Meta-Analysis. PLoS One. 2016;11(3):e0151653. Published 2016 Mar 17. doi:10.1371/journal.pone.0151653 [PubMed]
169. Powers JM, Buchanan GR. Disorders of iron metabolism: New diagnostic and treatment approaches to iron deficiency. Hematol Oncol Clin North Am. 2019 Jun;33(3):393-408. [PubMed abstract]
170. Manoguerra AS, Erdman AR, Booze LL, Christianson G, Wax PM, Scharman EJ, et al. Iron ingestion: an evidence-based consensus guideline for out-of-hospital management. Clin Toxicol (Phila) 2005;43:553-70. [PubMed]
171. Bergmann K, Bergmann OJAn unusual case of extreme thrombocytosis caused by iron deficiencyBMJ Case Reports CP 2020;13:e231833.
172. Lönnerdal B. Calcium and iron absorption–mechanisms and public health relevance. Int J Vitam Nutr Res. 2010;80(4-5):293-299. doi:10.1024/0300-9831/a000036 [PubMed][CrossRef]
173. Lynch SR. The effect of calcium on iron absorption. Nutr Res Rev. 2000;13(2):141-158. doi:10.1079/095442200108729043 [PubMed][CrossRef]
174. Ahern K., Rajagopal I., Tan T. Structure & Function- Amino Acids. LibreTexts Biology. https://bio.libretexts.org/Bookshelves/Biochemistry/Book%3A_Biochemistry_Free_For_All_(Ahern_Rajagopal_and_Tan)/02%3A_Structure_and_Function/202%3A_Structure__Function_-_Amino_Acids
175. Yi J, Thomas LM, Musayev FN, Safo MK, Richter-Addo GB. Crystallographic trapping of heme loss intermediates during the nitrite-induced degradation of human hemoglobin. Biochemistry. 2011;50(39):8323-8332. doi:10.1021/bi2009322 and RCSB PDB [PubMed]
176. Hubbard SR, Hendrickson WA, Lambright DG, Boxer SG. X-ray crystal structure of a recombinant human myoglobin mutant at 2.8 A resolution. J Mol Biol. 1990;213(2):215-218. doi:10.1016/S0022-2836(05)80181-0 and RCSB PDB [PubMed]
177. What Is Gut Dysbiosis? Cleveland Clinic. [Cleveland Clinic]