BUN: Diagnostic Significance and Clinical Insights
Authors: Payal Bhandari M.D.
Contributors: Nyah Zhang, Vivi Chador, Nigella Umali Ruguian

Key Insights
Proteins are vital for the body, serving roles in tissue building, substance transport, and chemical reactions. Since the body cannot store proteins, it continuously breaks them down and rebuilds them using amino acids, the building blocks of proteins. Of the many amino acids, 20 are essential for the human body but must be obtained through food as the body cannot produce them.
The blood urea nitrogen (BUN) test is a key biomarker that assesses nutritional status, protein metabolism, and overall health. It measures urea, a waste product of protein metabolism in the liver, which is normally filtered by the kidneys and excreted in urine. High blood urea levels can signal kidney or liver dysfunction, leading to oxidative stress, gene mutations, and reduced cell function. Impaired protein metabolism and waste excretion can cause severe conditions like vascular diseases, autoimmune disorders (e.g., diabetes), infections, cancers, and organ damage. Monitoring BUN levels supports early disease diagnosis and management.
What is BUN?
The blood urea nitrogen (BUN) test, also called the “BUN, serum” or “BUN, plasma” test, evaluates the balance between protein metabolism and the clearance of urea, a waste product formed when the liver converts toxic ammonium into less toxic urea. Urea is released into the bloodstream and excreted mainly in urine, with smaller amounts eliminated through sweat and stool.Excess urea in the blood acts as a pro-oxidant, contributing to oxidative stress, damaging cells, and mutating genes involved in protein and fat metabolism.
Proteins are composed of amino acids linked by peptide bonds. Each amino acid has an amino group (-NH2), a carboxyl group (-COOH), and a unique side chain (R). During protein metabolism, the toxic amino group (NH4+) binds to transport proteins like albumin for delivery to the liver or skeletal muscles. The liver repurposes NH4+ to create non-essential amino acids, while skeletal muscles use it for energy. Ammonia (NH3+) is eventually converted into urea (NH2+) with the release of carbon dioxide (CO2).
Approximately 40–50% of urea is excreted by the kidneys, 10% via sweat and stool, and the remainder stored in fat cells, skeletal muscles, and organs like the liver. Excess blood urea causes inflammation, oxidative stress, and cellular damage.

Figure 1: Urea is the principal nitrogenous end-product of protein metabolism. It is a small organic molecule comprising two amino (NH2) groups and a linked carbonyl (carbon-oxygen) group. The toxic amino group is broken down into ammonia in the liver and converted to less toxic urea with water, uric acid, and the waste product carbon dioxide (CO2) released. The lungs remove CO2 during exhalation.

Figure 2: 40 to 50 percent of the toxic byproducts of amino acid metabolism are removed by the kidneys in the urine, while 10 percent is eliminated in the sweat and stool.
Protein Metabolism and Synthesis
Unlike dietary fat, protein cannot be stored and must be continuously broken down into amino acids for energy or new protein synthesis. The body processes over 250 grams of protein daily, rebuilding the same amount. Excess undigested protein is converted to glycogen and stored as fat, with more than 90% of dietary protein broken down only to amino acids.
Of the hundreds of amino acids in nature, only 20 essential amino acids are critical for human protein synthesis.. Since the body cannot produce these essential amino acids, it is vital to replenish them through nutrient-rich meals, especially chlorophyll-rich plants, to prevent muscle protein breakdown for energy. Moreover, the body cannot produce essential amino acids.
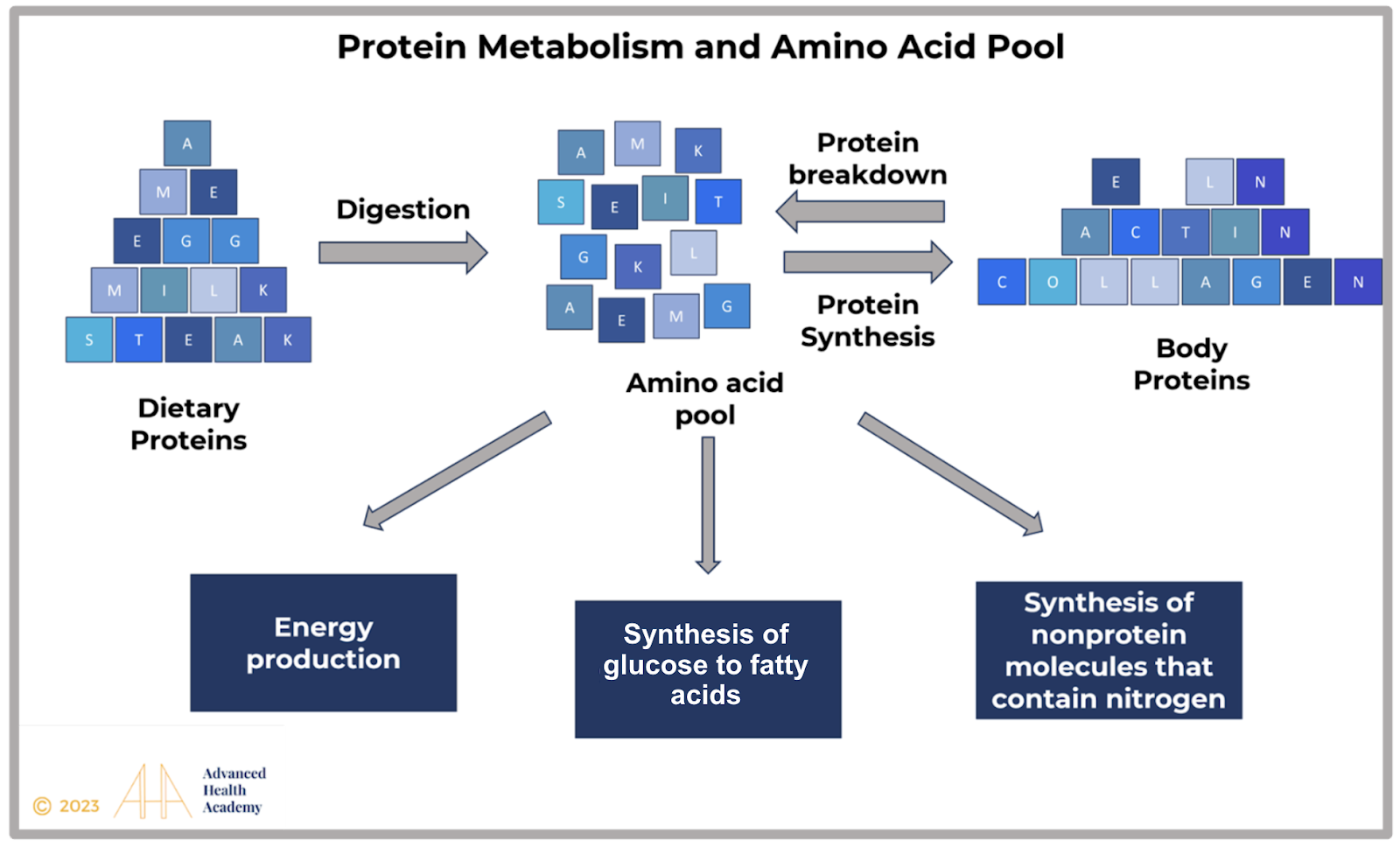
Figure 3: Amino acids derived from food and muscle protein metabolism are placed into a “pool” and used to form new proteins and other nitrogen-containing compounds.
When we chew food, healthy bacteria in the mouth react with saliva and convert 40 percent of the nitrates and nitrites in dietary protein to nitric oxide. Nitric oxide is transported from the mouth to the bloodstream. Nitric oxide keeps arteries flexible and young, maintains blood pressure, assists nerve cell communication, and prevents the growth of pathogenic microorganisms and mutated/abnormally functioning/cancer cells . The remaining undigested protein travels from the mouth through the esophagus to the stomach. Hydrochloric acid (HCl; 0.5 percent of stomach fluid) and the digestive enzyme pepsin create an acidity level (pH) of 1.5 to 3.5, which enables the breakdown of proteins into amino acids (AA) in the stomach and the formation of a uniform mixture called chyme. The greatest concentration of protein metabolism after that occurs in the small intestine, where bacteria release digestive enzymes (type of protein) secretin and cholecystokinin and cause the following cascade of reactions:
AAs break down into metabolic intermediates for harvesting energy by peripheral tissues and enabling normal physiological functions in the body ,
Nitrates and nitrites are converted to nitric oxide,
Essential vitamins and minerals are absorbed and transported to various organs and the bloodstream, which are also critical for harvesting energy and maintaining many critical functions,
Indigestible carbohydrates (like plant-derived dietary fiber) are converted to short-chain fatty acids (like acetate, propionate, and butyrate),
The pancreas releases sodium bicarbonate and digestive enzymes (such as trypsin, chymotrypsin, and elastase) to metabolize proteins further and neutralize HCl.

Figure 4: Ingested protein metabolism involves bacteria in the mouth and small intestine, stomach hydrochloric acid (HCl), and various digestive enzymes released from the stomach, small intestine, and pancreas. Proteins are broken down into amino acids, nitrates, and nitrites, then transported to the liver, various organs, and bloodstream. Sodium bicarbonate secreted by the pancreas protects the gut’s inside lining from being damaged by HCl. However, reduced protein metabolism decreases the synthesis of new proteins, such as enzymes, which are critical for digesting proteins, fats, and carbohydrates. Excess undigested food particles and their toxic metabolites in the gut can mount an inflammatory process that can damage surrounding tissues and blood vessels.

Figure 5: The conversion of nitrates and nitrites in dietary plant-based proteins to nitric oxide (NO) by healthy bacteria in the mouth, small intestine, and skin play a critical role in protecting blood vessels and various organs from injury and keeping inflammation, infections, and cancer growth under control. 40 percent of the nitrates and nitrites are converted to NO, while 60 percent is excreted in the urine. From the small intestine, nitrates and nitrites travel back to the mouth, are stored in the salivary glands or under the skin, and are converted by bacteria to NO.
Role of Nitrogen in the Body
All life on Earth requires nitrogen as it is an essential part of amino acids and nucleic acids – the building blocks of all living things. We breathe 80 percent nitrogen gas (N2) and 20 percent oxygen (O2). Plants and bacteria that synthesize energy from sunlight (photosynthesizers) are the primary producers of nitrogen. Plants cannot utilize N2, but bacteria can. Photosynthetic bacteria live in the soil and attach to plant roots on land. In water, these bacteria float freely. Certain photosynthetic bacteria contain the enzyme nitrogenase, which enables the conversion of N2 to ammonia (NH3) or ammonium (NH4). Through oxidation, certain bacteria turn NH4 into nitrite (NO2), while others convert nitrite (NO2) into nitrate (NO3).
Nitrate (NO3) is a more stable molecule than nitrite (NO2) and the best source of nitrogen for photosynthesizers. Nitrogen in the soil is transported from the roots to the chlorophyll in plant cells and used to convert sunlight into energy via cellular respiration. Energy comes in the form of high-energy electrons that harvest primarily adenosine triphosphate (ATP). Limited nitrogen in plants translates to limited chlorophyll production and photosynthesis, reducing available phosphate. Limited available chlorophyll-rich plants translate to less overall energy in the food web for sustaining all life on Earth. Therefore, reduced consumption of direct photosynthesis plants translates to reduced ATP and nitric oxide production, resulting in accelerated blood vessels and multi-organ damage.

Figure 6: Nitrogen continuously moves through the environment between living things, the soil, and the atmosphere. Nitrates (NO3), the most stable form of nitrogen commonly found in the soil, is transported through the roots to chlorophyll-rich plants grown above the ground, such as dark leafy vegetables (e.g., kale, arugula, swiss chard, spinach), beet and carrot greens, cabbage, cauliflower, and broccoli. Nitrates are not naturally found in animal products (like meat, shellfish, fish, and dairy) and, thus, are added by processing plants for the sole purpose of preservation.
Regulation of BUN Blood Levels
The body’s energy-harvesting capacity significantly impacts protein metabolism and BUN levels. Energy is primarily produced as adenosine triphosphate (ATP) via cellular respiration, which generates 34 ATP through the mitochondrial electron transport chain and 4 ATP from glycolysis and the Krebs cycle.
Typically, energy is harvested from glucose through glycolysis. However, during low-energy states (e.g., prolonged fasting or intense exercise), ketogenesis produces energy by breaking down stored proteins and fats into amino acids, lactic acid, and glycerol. This process occurs mainly in the liver and, to a lesser extent, in the kidneys and small intestine. Since the brain cannot use fat directly, glycerol from triglycerides must first convert into glucose.
Ketogenesis reduces the brain’s reliance on carbohydrates and proteins, curbs hunger, and stabilizes protein and glucose levels. It helps prevent excess fat accumulation in adipose tissue (obesity), blood vessels (atherosclerosis), and organs while supplying sufficient energy for physiological functions. It also supports the efficient clearance of toxic waste products like ammonia, urea, and nitrogen derivatives.

Figure 7: Cellular respiration is a set of metabolic reactions that convert electrons from plants that do direct photosynthesis into high-energy, electron-carrying molecules like adenosine triphosphate (ATP), nicotinamide adenine dinucleotide (NADH), and flavin mononucleotide-FMN (FADH), and release the waste product CO2 during exhalation by the lungs. Oxygen (O2) acts as the final electron acceptor, pulling down electrons in the electron transport chain and creating a proton gradient that drives energy (ATP) production.

Figure 8: The breakdown of fatty acids, amino acids, and glycerol in fat cells, the liver, and skeletal muscles regulates glucose and ketone production in the liver. Ketones provide an alternative energy source during prolonged fasting, intense exercise, insulin deficiency, or when the brain’s energy demand surpasses the body’s. Ketone synthesis produces significantly more energy (34 ATP) compared to glucose (2–4 ATP) and is strongly influenced by circadian rhythm (sleep-wake cycle) genes.
Clinical Significance of High BUN Test
Elevated blood urea nitrogen (BUN) levels indicate issues with protein metabolism in the digestive tract and liver, as well as reduced clearance of toxic waste products. High concentrations of ammonium, ammonia, and urea processed by the liver and kidneys elevate BUN and act as pro-oxidants, promoting glycolysis and ROS production while preventing ketogenesis. Insufficient healthy gut bacteria and excessive ROS disrupt protein and fat metabolism, reduce nitric oxide and nutrient availability, and damage the intestinal barrier. This leads to leaky gut syndrome, where undigested particles and toxins enter the bloodstream, triggering inflammation. White blood cells (WBCs) infiltrate to clear debris and heal tissues but release proinflammatory proteins and ROS, causing further damage, gene mutations, and impaired cell division. This systemic inflammation prompts the liver to increase glucose synthesis, break down skeletal muscle, and convert digested fats and proteins into stored fat, worsening metabolism. Elevated BUN levels correlate with vascular inflammation, dysfunctional blood cell activity, activation of dormant gut pathogens, and increased risk of mutated or cancerous cells.

Figure 9: Atherosclerosis-induced vascular inflammation involves hardening of arteries due to excess fat and plaque accumulation on the inside lining of blood vessels (hyperplasia tunica intima) and clot formation by leukocytes (white blood cells), thrombocytes (platelets), and endothelial smooth muscle cells. It restricts arterial blood flow, raises blood pressure, redistributes venous blood flow, and causes blood to back up into various organs, such as the heart, brain, lungs, and kidneys.
Persistent atherosclerosis is an inflammatory condition marked by rising proinflammatory proteins, oxidized LDL cholesterol, and toxic metabolites like urea in the bloodstream. These hinder oxygen delivery (hypoxia), disrupting energy production and tissue function. Blood flow backs up into organs like the kidneys, heart, lungs, and liver, enlarging and impairing their functionality. The lungs struggle to expel CO₂, while the liver and kidneys fail to clear toxins like ammonia and urea. A high BUN test often reflects kidney dysfunction, including poor fluid and electrolyte regulation, acid-base balance, and impaired vitamin D activation and red blood cell production. Dehydration from excess water and mineral loss worsens energy deficits and physiological dysfunction.
Excess heat overactivates WBCs, redirecting their focus from fighting foreign invaders to clearing tissue debris and repairing wounds. This can lead to WBCs attacking the body’s tissues, triggering autoimmune responses. High BUN levels are associated with dehydration and dysbiosis, weakening immune and reticuloendothelial systems, activating dormant pathogens, and promoting infections, cancer, autoimmune disorders, and multi-organ damage. Chronic kidney dysfunction also heightens susceptibility to medication side effects, exacerbating health issues. ,
Clinical Significance of Low BUN Blood Test
Reduced blood urea nitrogen (BUN) levels indicate lower production of protein metabolites like urea and free nitrogen. This can result from a low-protein diet or increased urea loss in urine. Pregnancy commonly lowers BUN levels due to fluid redistribution diluting blood urea and metabolic adaptations to meet maternal and fetal energy demands.
During pregnancy, maternal nitrogen primarily supports lean body mass, with reduced total protein and amino acid levels suggesting increased amino acid uptake by digestive organs, liver, and kidneys. Decreased urea synthesis tightly regulates protein and nitrogen metabolism to protect the mother and fetus from harmful pro-oxidant levels.
Pathological causes of low BUN include insufficient intake of nutrient-dense plant foods or hypersensitivity to protein-rich foods like animal products, nuts, or pesticide-resistant crops. Low stomach acid and reduced gut bacteria also impair protein metabolism and energy harvesting, increasing ROS and mutating enzymes involved in urea synthesis, further reducing BUN levels.
Conclusion
The blood urea nitrogen (BUN) test is a key biomarker of overall health, measuring urea, a waste product of protein metabolism in the liver. Urea is released into the bloodstream, filtered by the kidneys, and excreted in urine. Kidney or liver disease can impair urea excretion, raising BUN levels. Excess urea is stored in fat cells, skeletal muscles, and organs like the liver, acting as a pro-oxidant that damages cells, mutates genes, and disrupts fat metabolism, the body’s primary energy source during fasting.
Dehydration is the most common cause of abnormal BUN levels, leading to higher blood pressure, restricted arterial flow, and resource shifts to damaged tissues. High protein intake, particularly from animal sources, and inadequate plant-based foods can disrupt protein and fat metabolism, reduce nitric oxide, and increase BUN. Long-term medication use can also impair metabolism and elevate BUN.
Balanced BUN levels are crucial for preventing inflammatory conditions like vascular diseases, autoimmune disorders (e.g., diabetes), infections, cancers, and organ damage. Proper hydration, a plant-forward diet, intermittent fasting, and medication adjustments can help regulate BUN levels. Regular monitoring provides valuable insights for diagnosis, treatment, and management.
Source References and Supplemental Research
Pagana KD, Pagana TJ, Pagana TN. Mosby’s Diagnostic and Laboratory Test Reference. 15th ed. St. Louis, MO: Elsevier; 2021.
“Comparisons of hazard ratios when laboratory results were within the normal range demonstrated that blood albumin and blood urea nitrogen (BUN) were both negatively associated with mortality and alkaline phosphatase (AP) was positively associated with mortality.” Hu G, Duncan AW. Associations between selected laboratory tests and all-cause mortality. J Insur Med. 2013;43(4):208-220. [PubMed]
Increased discharge serum urea (> 16 mg/dL) was a predictor of increased mortality in heart failure patients. Gotsman I, Zwas D, Planer D, Admon D, Lotan C, Keren A. The significance of serum urea and renal function in patients with heart failure. Medicine (Baltimore). 2010;89(4):197-203. [PubMed]
A steady increase in mortality was predicted for Medicare patients (aged > or = 65 years) who were hospitalized for myocardial infarction (n = 44,437) who had increased levels of BUN > 17 mg/dL(> 6.1 mmol/L), creatinine > 1.0 mg/dL (> 88.4 micromol/L), and eGFR < 100 mL/min per 1.73 m2 and in patients who experienced heart failure who had increased levels of BUN > 16 mg/dL (> 5.7 mmol/L), creatinine > 1.1 mg/dL (> 97.2 micromol/L), and a Mayo eGFR <= 90 mL/min per 1.73 m2. Smith GL, Shlipak MG, Havranek EP, et al. Serum urea nitrogen, creatinine, and estimators of renal function: mortality in older patients with cardiovascular disease. Arch Intern Med. 2006;166(10):1134-1142. [PubMed]
A BUN ≥ 30 mg/dL was associated with a nearly 2-fold increased risk of mortality…” Sullivan DH, Sullivan SC, Bopp MM, Roberson PK, Lensing SY. BUN as an Independent Predictor of Post-Hospital-Discharge Mortality among Older Veterans. J Nutr Health Aging. 2018;22(7):759-765. [PubMed]
https://www.earth.com/earthpedia-articles/why-is-the-nitrogen-cycle-so-important/
Watford M. The urea cycle: Teaching intermediary metabolism in a physiological setting. Biochem Mol Biol Educ 2003; 31, 5: 289-97.
Lamb E et tal. Kidney Function Tests (Chapter 25) In: Tietz Textbook of Clinical Chemistry and Molecular Diagnostics. By: Burtis CA, Ashwood ER, Bruns DE. Elsevier Health Sciences; 2012. Available from: URL:https://books.google.dk/books?id=BBLRUI4aHhkC.
Bowker LK et tal. Raised blood urea in the elderly: a clinical and pathological study. Postgrad Med J 1992; 68, 797: 174-79.
Chung J et tal. P15 Elevated urea in the elderly: Age or EGFR – a database analysis. [cited 2015 Nov 26]. Available from:www.aacb.asn.au/documents/item/960.
Musch W et tal. Age-related increase in plasma urea level and decrease in fractional urea excretion: clinical application in the syndrome of inappropriate secretion of antidiuretic hormone. CJASN 2006; 1, 5: 909-14.
Witting MD et tal. ED predictors of upper gastrointestinal tract bleeding in patients without hematemesis. Am J Emerg Med 2006; 24, 3: 280-85.
Aronson D et tal. Elevated blood urea nitrogen level as a predictor of mortality in patients admitted for decompensated heart failure. The Am J Med 2004; 116, 7: 466-73.
Mehta AR. Why does the plasma urea concentration increase in acute dehydration? Advances in physiology education 2008; 32, 4: 336.
Kalhan SC. Protein metabolism in pregnancy. Am J Clin Nutr 2000; 71, 5 Suppl: 1249S-55S.
Salek J et tal. Recurrent liver failure in a 25-year-old female. Liver transplantation: official publication of the American Association for the Study of Liver
Diseases and the International Liver Transplantation Society 2010; 16, 9: 1049-53.Gao, X., Lee, H. Y., Li, W., Platt, R. J., Barrasa, M. I., Ma, Q., … & Lodish, H. F. (2017). Thyroid hormone receptor beta and NCOA4 regulate terminal erythrocyte differentiation. Proceedings of the National Academy of Sciences, 114(38), 10107-10112.
ROSE WC. The amino acid requirements of adult man. Nutr Abstr Rev. 1957 Jul;27(3):631-47.
Benjamin O, Lappin SL. StatPearls. StatPearls Publishing; Treasure Island (FL): Jul 19, 2022. Kwashiorkor.