GGT (gamma-glutamyltransferase): Diagnostic Significance and Clinical Insights
Authors: Payal Bhandari M.D., Amer Džanković, Madison Granados
Contributors: Hailey Chin, Vivi Chador, Nigella Umali Ruguian
Key Insights
The liver, known as the body’s “chemical factory,” processes proteins, fats, and cholesterol, supports energy production, detoxification, hormone regulation, and blood clotting. Liver function tests (LFTs) measure markers like ALT, AST, and GGT to assess liver health and metabolic function 1,2 3.
GGT, a key liver biomarker, can indicate alcohol misuse, liver damage, and conditions like diabetes, heart disease, or cancer. Certain medications, supplements, and substances like alcohol or steroids can harm the liver 4, 5, 6.
Liver diseases like fatty liver or hepatitis often show no symptoms until advanced. Regular GGT testing aids early detection, monitors treatment, and highlights risks from chronic inflammation and tissue damage 7.
What is GGT?
Gamma-glutamyl transferase (GGT) processes glutathione (GSH), a key antioxidant, and detects inflammation and disease. Low GGT levels, though rare, are linked to conditions like gastric and cervical cancer, preeclampsia, and anemia, often due to oxidative stress 9 10.
Cancer, the second leading cause of U.S. deaths, saw 1.96 million cases and 600,000 deaths in 2023. GGT helps detect and track aggressive cancers like pancreatic and liver, distinguishing liver cancer from other diseases 10 11 12 13.
GGT also identifies liver and brain dysfunction tied to poor diet, alcohol, tobacco, and inactivity. Monitoring GGT supports early detection, highlights lifestyle impacts, and reduces medication needs.
GGT’s Role in the Body
GGT is a vital enzyme involved in recycling and managing glutathione (GSH), the most abundant water-soluble antioxidant in cells, essential for many key functions in plants, animals, and humans 14 15 .
Maintain mitochondria, the cell’s energy producer (ATP) and protector against damage from oxidative stress caused by reactive oxygen species and inflammatory proteins like cytokines.16
Acts as a cofactor for liver enzymes that metabolize and excrete xenobiotics, including drugs and heavy metals.17
Eliminates toxic substances like reactive oxygen species (ROS), free radicals, peroxides, and heavy metals.17 18
Maintain adequate levels of exogenous antioxidants vitamins C and E20,21,22
Supports DNA, protein, and cellular repair, aids immune and nerve function, transports amino acids, and promotes cell health and longevity.23
Regulates glutamate and GABA levels in the brain. GABA, the main inhibitory neurotransmitter, supports sleep, mood, blood pressure, pain perception, and precise nerve function.27 28
Studies show that mice without hepatic GSH synthesis die within a month, highlighting the importance of GSH in critical processes like digestion, DNA replication, respiration, and muscle and nerve function. Low GSH levels increase the risk of premature aging, cancer, heart disease, neurodegenerative disorders, and autoimmune conditions. 29,30
Physiology of GGT
Origin and Formation of GGT
The enzyme gamma-glutamyl transferase (GGT) is a protein that binds substrates through active sites.31. Activation requires structural changes or the addition of a carbohydrate to a specific amino acid. Translated from chromosome 22, GGT consists of 569 amino acids 31 32 33. Mutations in GGT-related genes can significantly impact cell health and metabolic processes.
Synthesis of Glutathione
Glutamate-cysteine ligase converts glutamate and cysteine into gamma-glutamylcysteine, and glutathione synthetase adds glycine to form glutathione (GSH). In the liver, kidneys, pancreas, and bile ducts, GGT breaks GSH into amino acids for resynthesis and energy production. The gamma-carboxyl group in Glu bonds with cysteine, making GSH resistant to enzymes and ROS. Since cysteine is the least abundant amino acid, GGT and the gamma-glutamyl cycle are vital for GSH metabolism, especially during cysteine shortages 34 35 36.
GSH Regulation
GSH is regulated by SAH, SAMe, and vitamins B6, B9, and B1237. Deficiencies in B vitamins or imbalances in SAH and SAM increase GSH breakdown by GGT, releasing hydrogen sulfide (H2S). Elevated H2S and GGT levels disrupt the production of key molecules, detoxification, drug metabolism, and energy production.
GSH regulation involves the following steps:
After eating a methionine-rich meal (found in animal products, nuts, and oils), ATP adds an adenosyl group to methionine, a reaction catalyzed by methyltransferase.
SAMe donates methyl groups to DNA, RNA, and proteins, producing S-adenosyl-homocysteine (SAH).
SAH is rapidly broken down by the enzyme SAH hydrolase into adenosine and homocysteine (Hcy).38, 17 .
Hcy enters the bloodstream, binds to albumin, and is mostly reabsorbed by the kidneys, with only 1% excreted in urine.
Inside cells, Hcy can be remethylated back to methionine using vitamin B9 (folate) and vitamin B12 with the enzyme methionine synthase39.
Alternatively, Hcy combines with serine to form cystathionine, catalyzed by the enzyme cystathionine beta-synthase (CBS) and vitamin B6. Cystathionine is then broken down by cystathionine gamma-lyase (CGL) into cysteine, alpha-ketobutyrate, and ammonia.
Cysteine is further processed into glutathione (GSH) and hydrogen sulfide, both essential for cellular function and antioxidant defense.
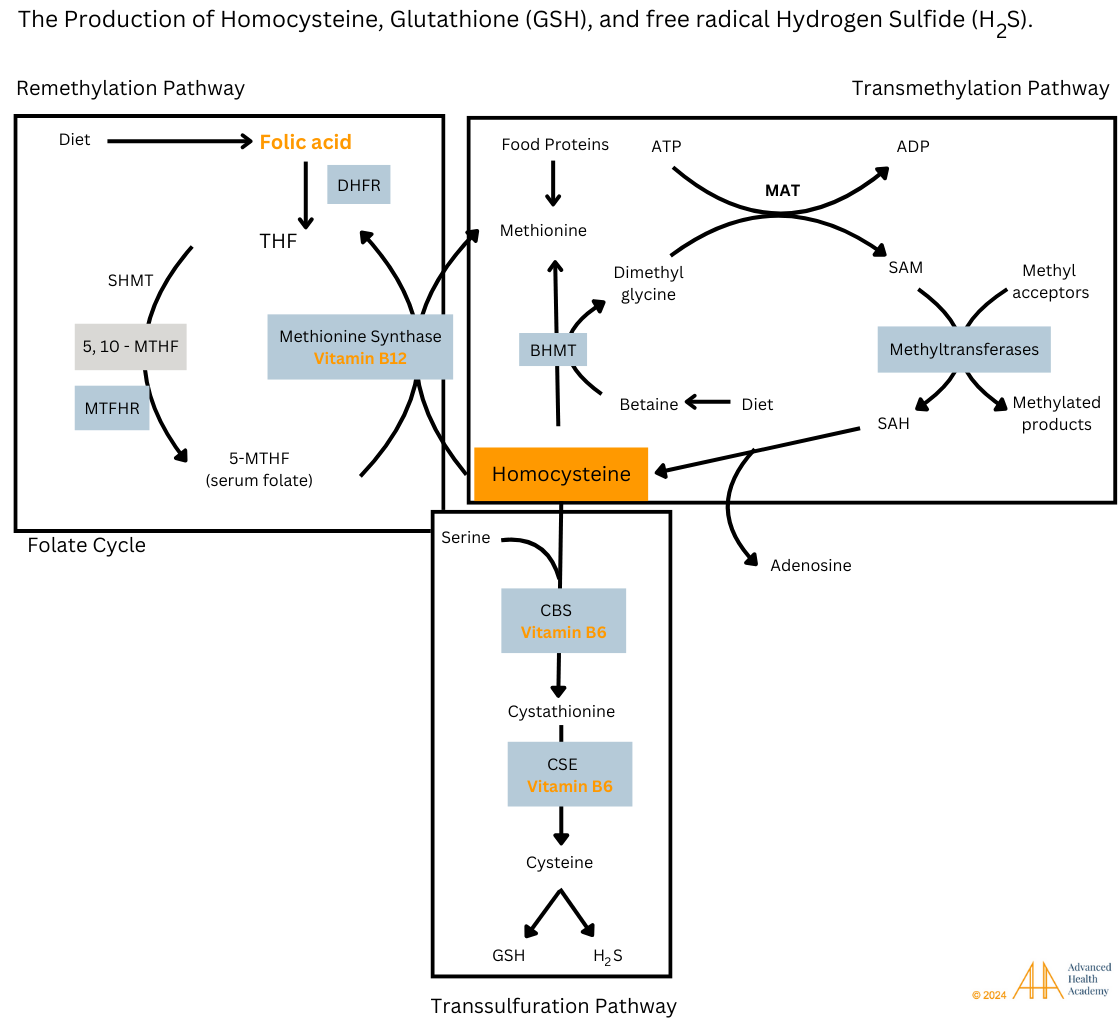
Figure 1: Homocysteine (Hcy) inside cells follows two main pathways: it is either converted back to methionine or transformed into cysteine and glutathione (GSH). These processes are regulated by S-adenosyl-methionine (SAM) and S-adenosyl-homocysteine (SAH), along with vitamins B6, B9, and B12. Deficiencies in these vitamins can disrupt GSH production, increasing its breakdown and releasing harmful free radicals like hydrogen sulfide (H2S).40
GGT Regulation
The liver is essential for processing proteins, amino acids, fats, and cholesterol, producing enzymes, balancing hormones and energy, and detoxifying waste. GGT levels in the blood are influenced by factors like age, gender, hormones, diet, medications, and substances that can harm the liver, as well as the kidneys, pancreas, and bile ducts where GGT is also found41.
Hormones
Insulin supports converting homocysteine (Hcy) to methionine, reducing cysteine and glutathione (GSH) production, and lowering GGT activity42. It also boosts fat metabolism and energy (ATP) production, essential for cell health and reducing harmful reactive oxygen species (ROS). In contrast, insulin deficiency raises blood sugar, increases Hcy levels, reduces cysteine production, and elevates ROS 43. This damages cells, lowers GSH levels, and increases GGT activity.
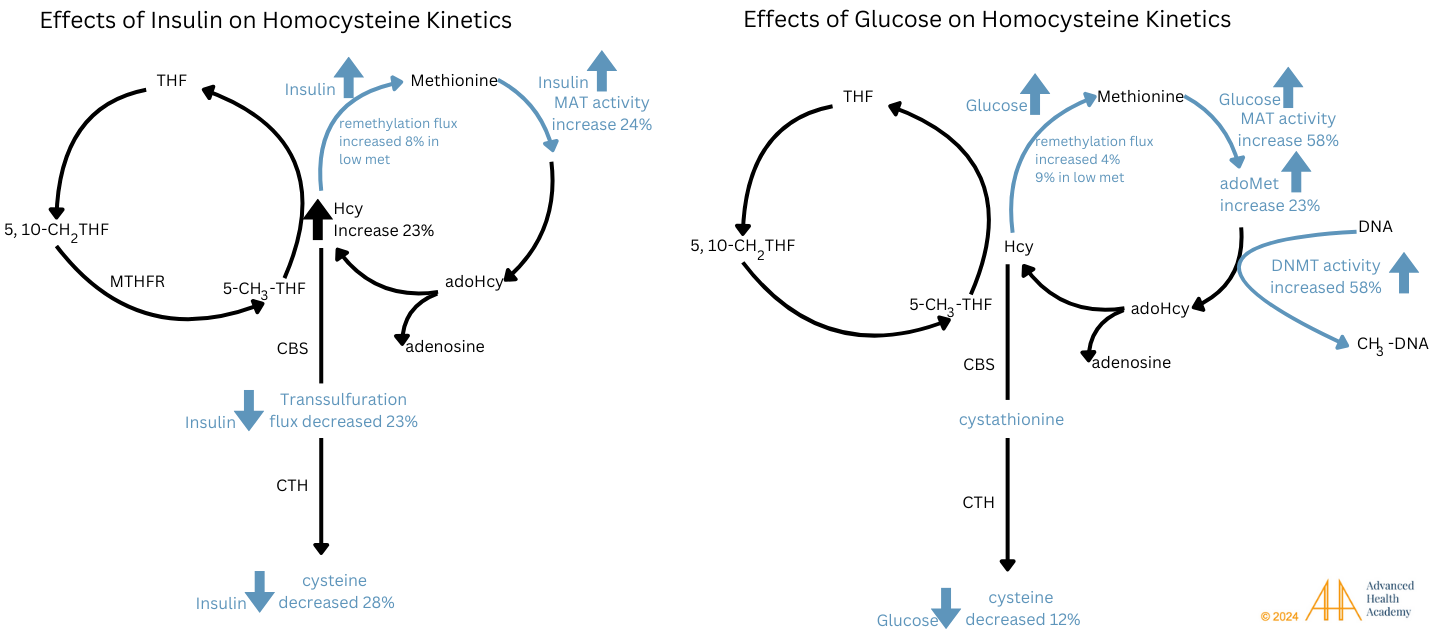
Figure 2: Higher insulin levels increase transmethylation, raising homocysteine (Hcy) levels and reducing cysteine. When methionine is low, insulin boosts Hcy by promoting its conversion to methionine. High blood glucose also promotes methionine remethylation, further increasing Hcy levels. These processes reduce glutathione (GSH) production, linking elevated insulin, glucose, and Hcy to lower GSH levels.44
Thyroid hormones
Hyperthyroidism or prolonged synthetic thyroid hormone use affects liver function, with 24% showing altered GGT levels. The thyroid and liver regulate energy, DNA activation, protein synthesis, oxygen use, and heat. Thyroid hormones T4 and T3, activated in the liver, support metabolism, clear toxins, aid blood vessel formation, and may influence cancer growth 45 46 .
A review (2000–2021) linked liver disease and thyroid toxicity to heart failure and Graves’ disease. Antithyroid treatments normalized GGT in 70% of cases and improved markers like ALT and AST. Monitoring these biomarkers helps detect diseases, track health, and guide treatment 45.
Environmental Toxins
Smoking disrupts blood flow, overstimulates the HPA axis, and raises cortisol, increasing blood glucose and inflammation. Cadmium in nicotine triggers inflammatory proteins, reduces energy, and raises ROS, which damages cells, elevates GGT, depletes glutathione, weakens vitamins C and E, and lowers serotonin and melatonin, impacting mood and sleep 47, 48.
Alcohol impacts DNA methylation of liver genes like alcohol dehydrogenase. Excess acetaldehyde increases homocysteine (Hcy) conversion to methionine but reduces glutathione (GSH), allowing ROS to damage liver cells and raise GGT levels. Chronic alcohol use can cause liver inflammation, scarring, and cirrhosis. Reducing alcohol intake supports GSH and prevents ROS damage 49.
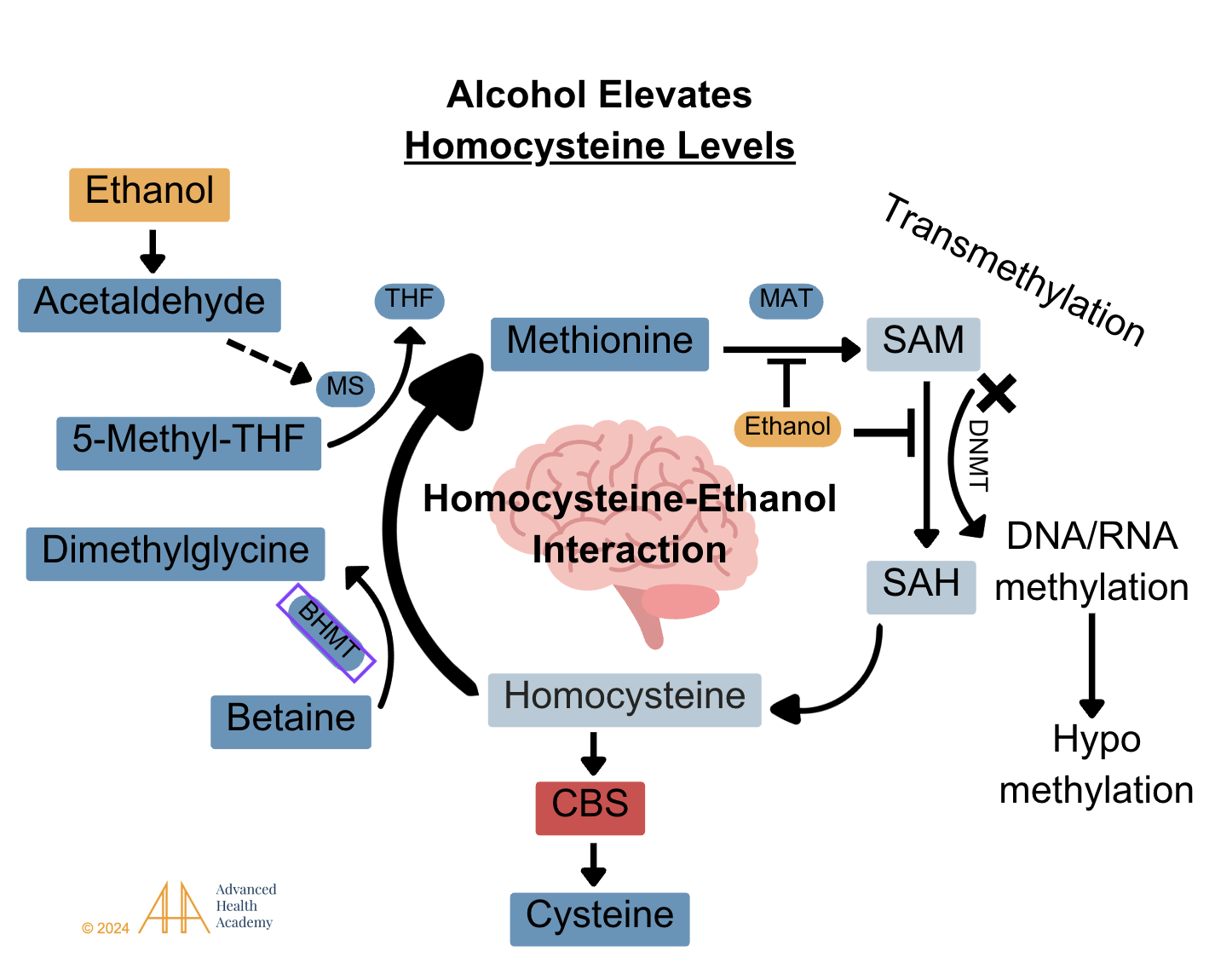
Figure 3: Acetaldehyde, a byproduct of alcohol, disrupts the balance of SAM and SAH, increasing homocysteine (Hcy) conversion to methionine while reducing cysteine and glutathione (GSH) production. Lower GSH levels allow reactive oxygen species to damage liver cells, raising GGT levels.
Chemical solvents and heavy metals can harm liver health, especially with prolonged occupational exposure in industries like healthcare, farming, and dry cleaning.50 Substances like trichloroethylene, carbon tetrachloride, toluene, and heavy metals like mercury and cadmium can cause liver damage, including hepatitis, steatosis, and fibrosis 51 52 53. Cadmium, in particular, damages mitochondria, reducing energy production.53 Heavy metals enter the body through contaminated food, water, alcohol, smoking, fumes, or skin contact. It’s essential to handle these chemicals cautiously and inform healthcare providers of any exposure.
Pharmaceutical Medications
Long-term drug use can impair vitamin absorption and disrupt metabolic pathways. Liver-metabolized medications deplete heme iron, reducing oxygen and nutrients to other organs. Certain drugs affect methylation and transsulfuration cycles, increasing tissue damage and reactive oxygen species. Regularly review medication use and dosage, especially with abnormal GGT levels.
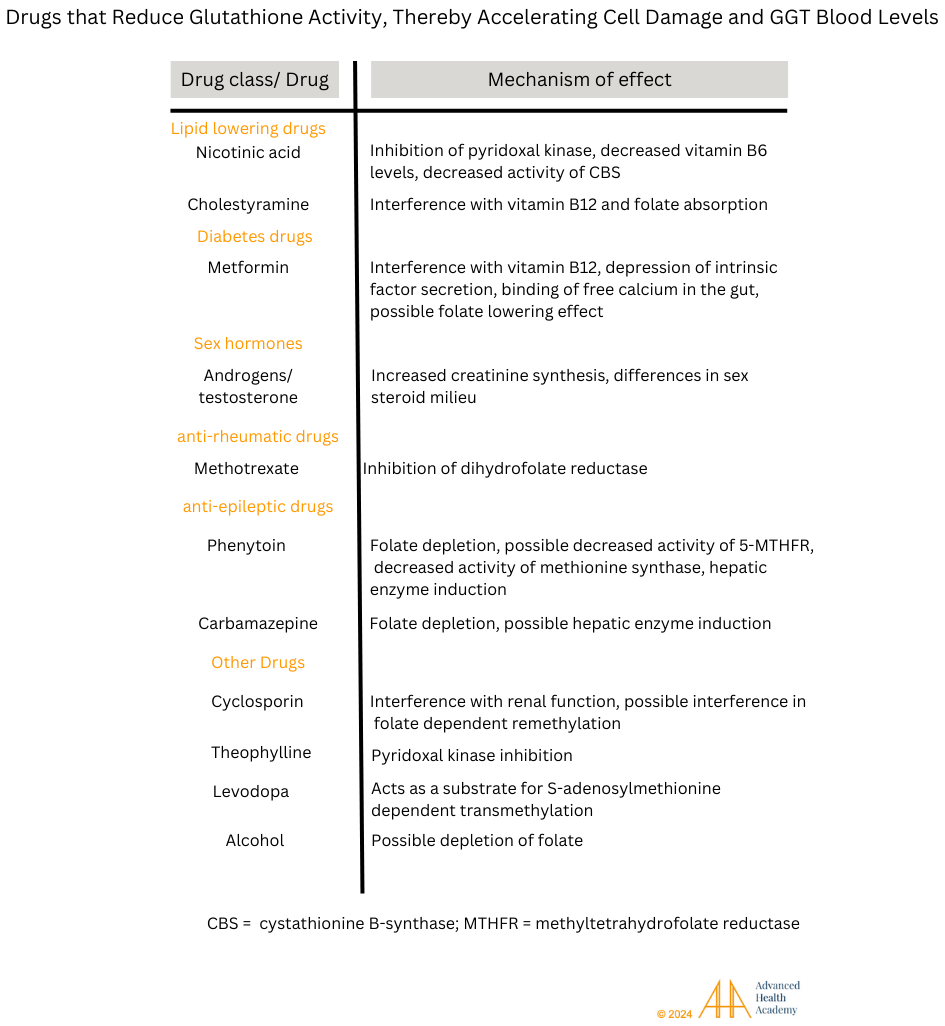
Table 1: Drugs affecting liver and digestive metabolism can disrupt transmethylation and transsulfuration, raising GGT activity. This leads to glutathione depletion and increased hydrogen sulfide, causing tissue damage in multiple organs54.
Drug-induced liver injury (DILI) is the leading cause of acute liver failure in the U.S. and Europe and can be fatal 55, 56. It is also a major reason for drug withdrawals from the market and research. DILI is categorized into intrinsic and idiosyncratic types.
Intrinsic DILI is predictable and observed in preclinical studies 57, 58. For instance, taking over 7.5 g of acetaminophen (APAP) in a single dose can cause acute liver toxicity. Even the recommended dose of 4 g/day for two weeks can elevate liver enzymes like ALT to three times the normal limit in about one-third of patients 59.
Idiosyncratic DILI (IDILI) is unpredictable, not dose-dependent, and may take weeks or months to develop. It causes 10–15% of acute liver failure in the U.S. Factors like disrupted gut microbiota, chronic anemia, and excess ROS increase the risk of drug interactions leading to systemic allergic reactions. Repeated drug use worsens liver injury over time 60 61 62.
DILI often mimics acute viral liver infections and lacks skin symptoms, making diagnosis challenging. Its clinical and histological features resemble other liver disorders, reducing the usefulness of biopsies. Considering drug involvement is crucial.
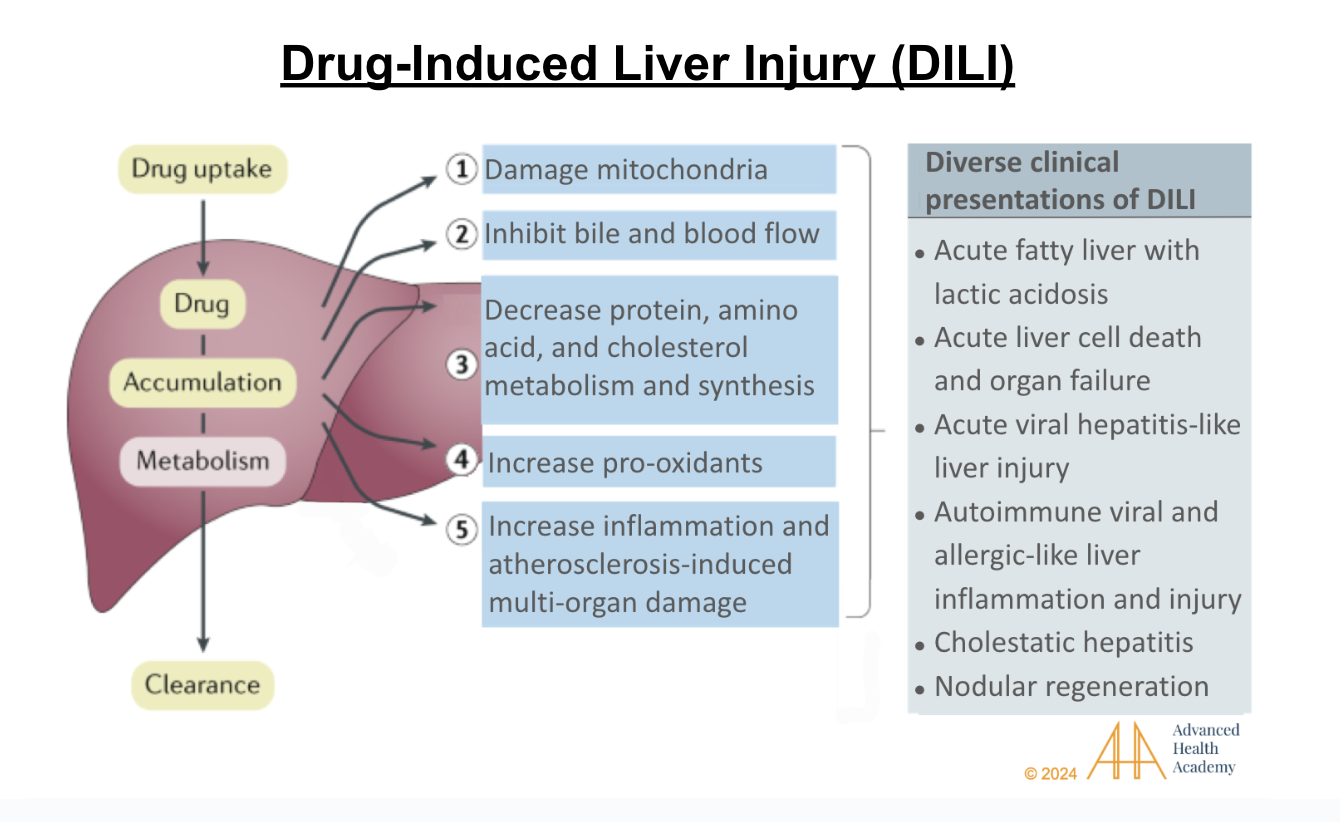
Figure 4: Drug-Induced Liver Injury. The accumulation and metabolism of drugs in the liver can cause a variety of pathophysiologic complications that often go undiagnosed as DILI.
Clinical Significance of Monitoring High GGT Levels
GGT is a noninvasive biomarker linked to various health conditions and overall survival. High GGT levels often indicate vitamin B6, B9, or B12 deficiencies, reduced antioxidant activity, and increased reactive oxygen species (ROS). ROS can mutate genes, such as those for cystathionine-β-synthase (CBS), decreasing cysteine production and raising homocysteine (Hcy) levels. Low cysteine storage triggers higher GGT production in the liver, pancreas, kidneys, and bile ducts. Elevated GGT degrades glutathione (GSH), releasing harmful hydrogen sulfide and reducing antioxidant and mitochondrial activity 63 64 35.
Atherosclerosis-Induced Vascular Inflammation
Abnormal GGT levels are often linked to lifestyle factors. Dysbiosis and reduced blood flow disrupt gut microbiota, impairing digestion, nutrient absorption, and waste excretion. Nutrient deficiencies affect metabolism, protein synthesis, and fat-soluble vitamins (A, D, E, K). Undigested food entering the bloodstream increases blood viscosity, causing hypoxia. 67, 68. The liver responds by producing glucose, storing fat, and slowing fat breakdown. Excess fat and ROS damage cells, causing inflammation 69, 70.
Oxidized LDL cholesterol deposits in damaged vessels attract immune cells, forming plugs of fat and scar tissue. This restricts blood flow, raises blood pressure, and impairs organ function 71 72.
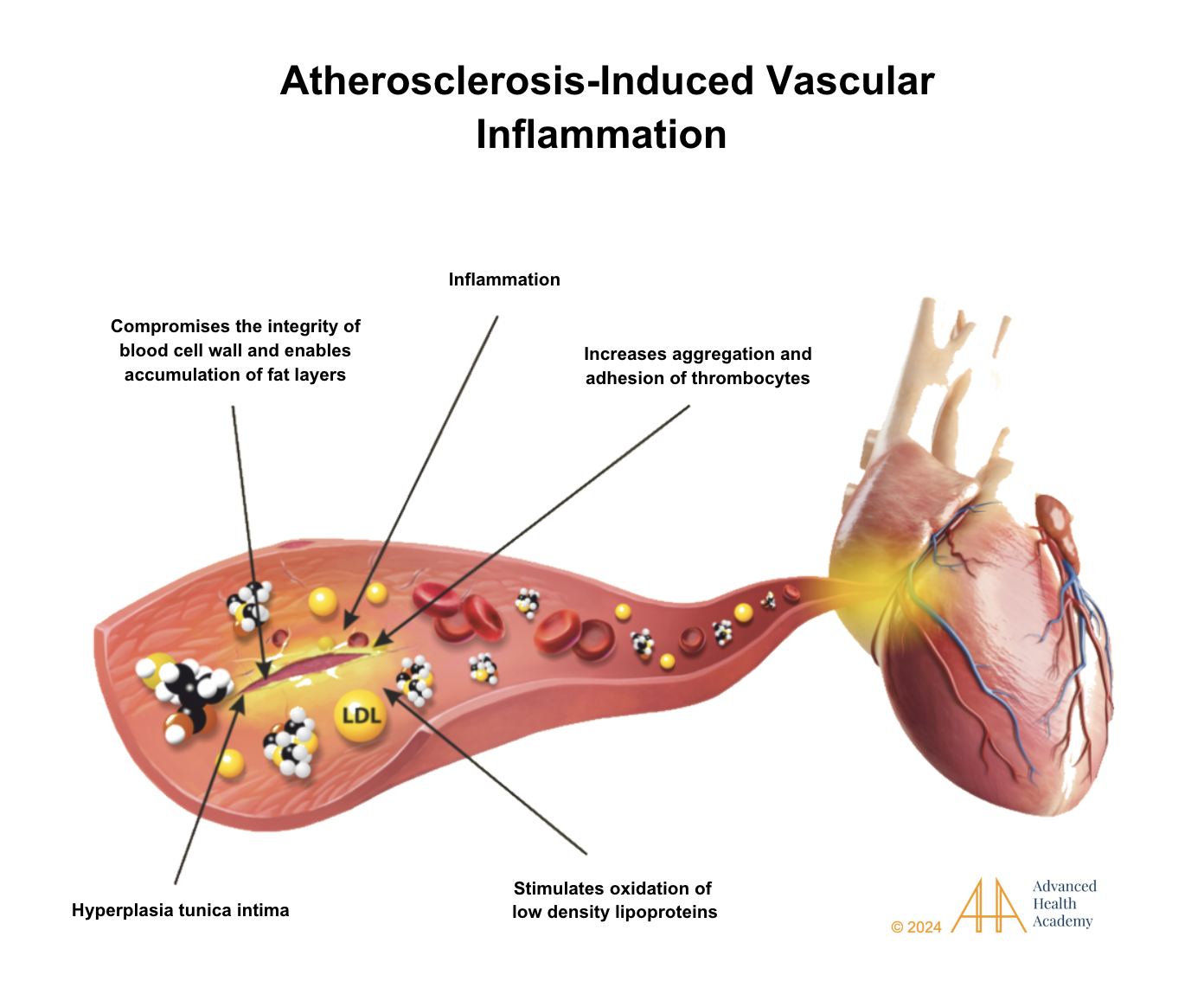
Figure 5: Atherosclerosis-related vascular inflammation involves artery thickening (plaque buildup), oxidized LDL cholesterol, and platelet-induced clot formation.
Atherosclerosis creates a cycle where excess ROS and inflammatory proteins mutate genes, disrupt energy and hormone balance, and activate WBCs and platelets. WBCs, focused on clearing debris and repairing tissue, may attack healthy cells, triggering autoimmune inflammation and altering organ function. WBCs and platelets also work with pathogens and tumor cells to absorb free cholesterol, heme, and iron, deposit scar tissue, form clots, and build new blood vessels 73 74, 75.
Monitoring GGT levels helps detect and track diseases like atherosclerosis, autoimmune disorders, infections, cancer, and organ damage. While often treated with medications, these conditions can be prevented or managed through lifestyle changes like a healthy diet, hydration, intermittent fasting, and stress reduction. ROS levels directly influence gene expression and health outcomes.
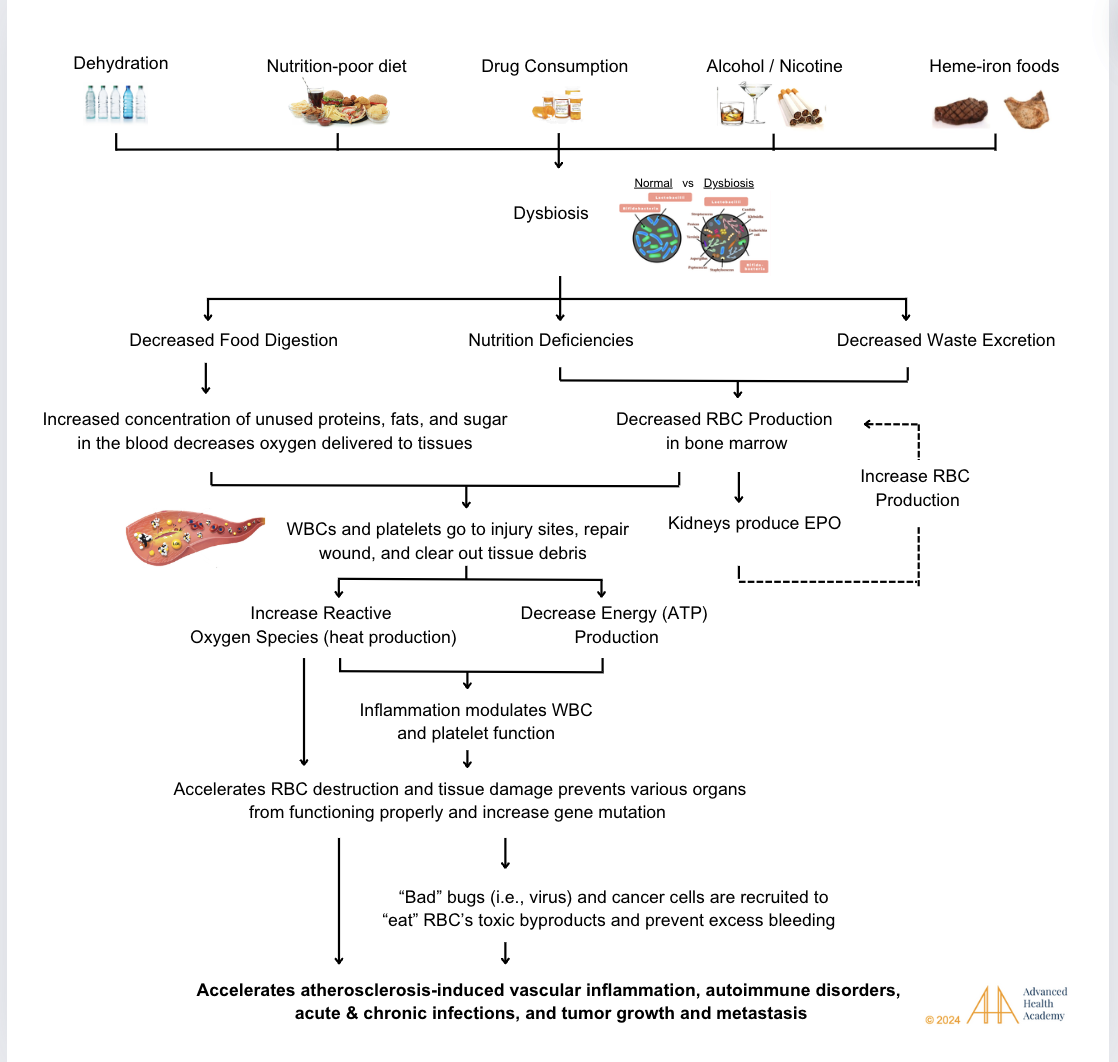
Figure 6: Chronic inflammation increases ROS, damaging liver cells and raising GGT levels, which heightens the risk of hypoxia-related tissue damage. Key causes include dehydration, nutrient-poor heme-rich diets, and substances like alcohol, tobacco, and certain medications that impair blood flow and accelerate cellular aging.
Liver and Brain Dysfunction
When oxygen levels drop below 2%, the liver reduces hemoglobin production, leading to hypoxia, impaired energy production, and increased red blood cell (RBC) destruction.76 Chronic liver damage is linked to processing RBC byproducts like hemoglobin, iron, and cholesterol, which accumulate in organs like the liver, pancreas, and bone marrow, disrupting metabolism. Excess bile, a heme byproduct, can form gallstones, block bile flow, damage the liver and bile ducts, and raise GGT and ROS levels. Bile can also harm the intestine, cross the blood-brain barrier, and trigger neurological and systemic inflammation77.
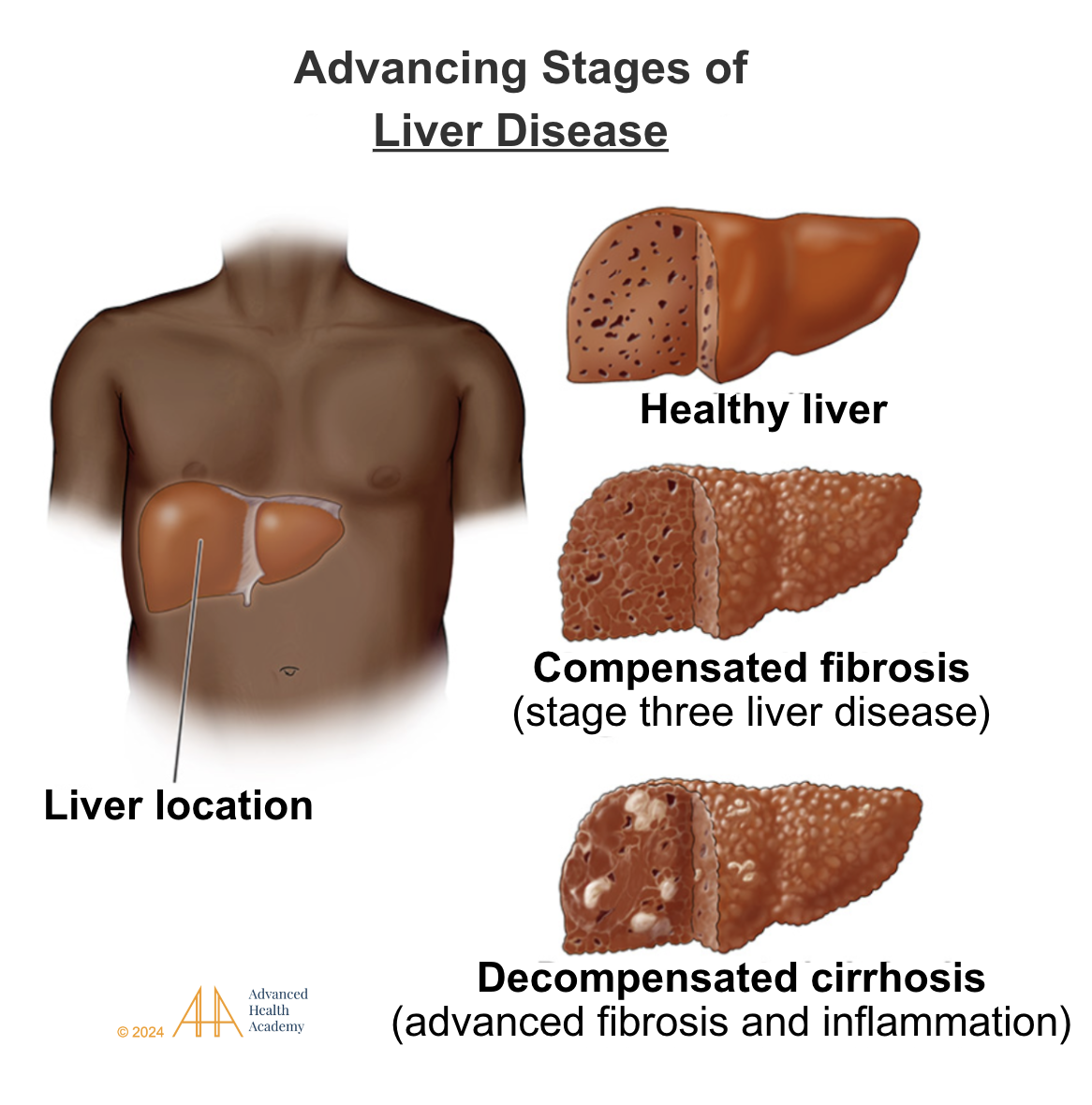
Figure 7: Chronic liver disease (steatosis, steatohepatitis, and cirrhosis) is linked to excess inflammatory proteins and fat deposits, which disrupt energy production and metabolism. Chronic inflammation increases reactive oxygen species, damaging organ structure and function.
Glutamine, the most abundant amino acid, is found in much higher concentrations in plasma and tissues than other amino acids. 78 The liver regulates pH, protein synthesis, and detoxification. In muscles, the spinal cord, and the brain, the liver enzyme glutamine synthetase converts glutamate and ammonia (a toxic byproduct) into glutamine, protecting against ammonia toxicity. 78 The enzyme glutaminase in the liver breaks glutamine into glutamate and ammonium ions, which are excreted as urea through urine. 78
Chronic liver inflammation disrupts protein and amino acid metabolism, increasing ammonia and GGT levels. This triggers brain inflammation, leading to symptoms like hyperactivity, seizures, altered consciousness, encephalopathy, coma, and psychomotor issues.79 80,81
Cancer Growth and Metastasis
Elevated GGT levels degrade glutathione (GSH), increasing hydrogen sulfide (H2S) production and reducing antioxidant activity. H2S promotes DNA methylation and protein production for cancer growth, creating oxidative stress that activates platelets and white blood cells. These cells, along with pathogens and cancer cells, ingest excess heme-iron, oxidize proteins and cholesterol, form clots, and build new blood vessels. High GGT levels are linked to a higher risk of infections, cancer growth, and metastasis.
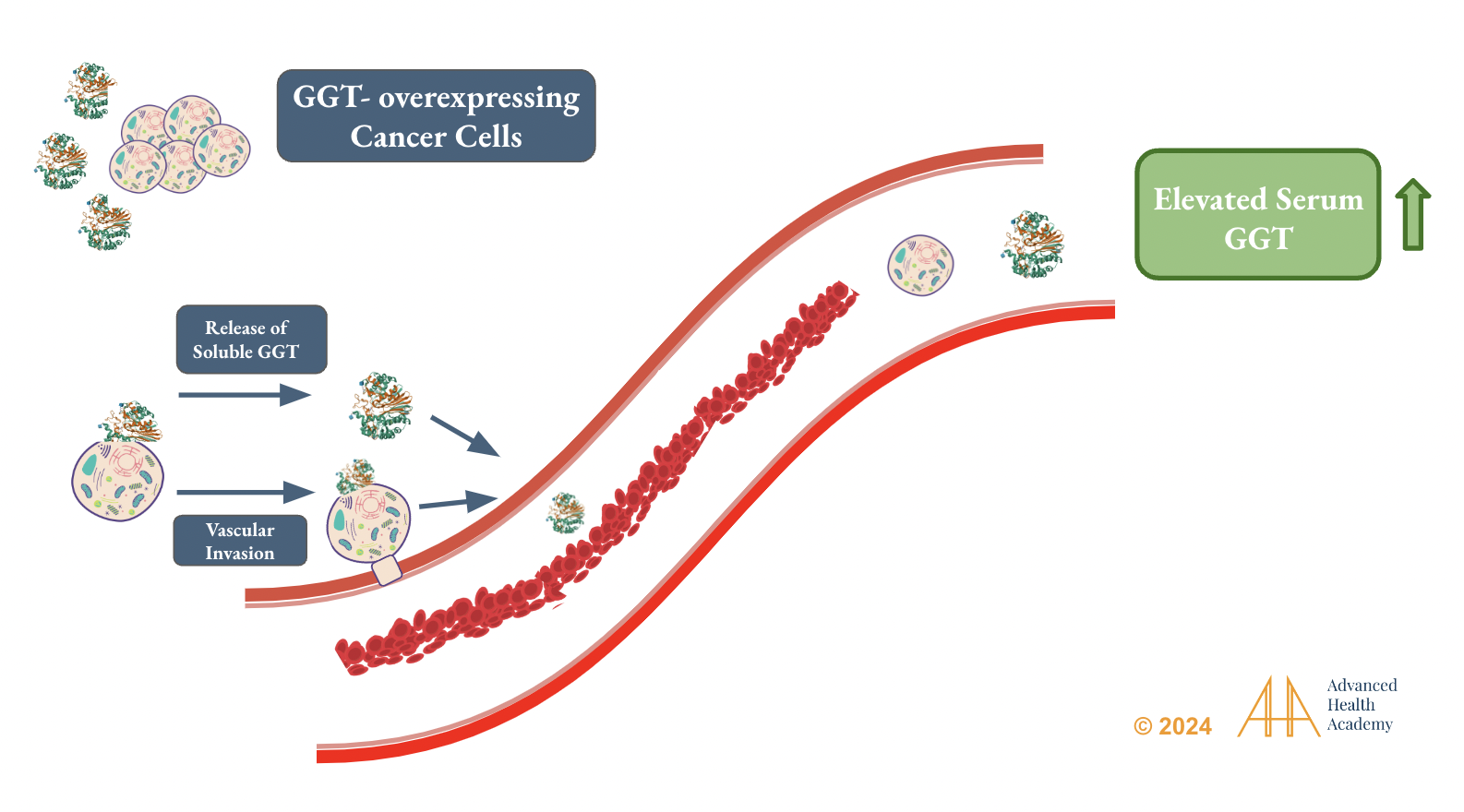
Figure 8: Cancer cells produce GGT, depleting glutathione and increasing ROS, which damages cells and disrupts metabolism. This diverts white blood cells and platelets from fighting cancer and pathogens, promoting tumor growth and metastasis.
Clinical Significance of Monitoring Low GGT Levels
Low GGT levels generally indicate good mental and physical health, reflecting adequate glutathione levels, balanced vitamin and mineral intake, and a plant-forward diet. Reduced dietary protein from animal sources, nuts, and legumes can enhance GGT metabolism and lower levels. Low or moderate alcohol consumption also keeps GGT levels down, as higher intake is linked to fatty liver disease. Since GGT is involved in protein metabolism, waste excretion, and energy production, low levels may result from dietary, lifestyle, environmental, medication, or genetic factors. GGT levels should be assessed alongside overall health and other liver biomarkers.
Conclusion
The liver processes nutrients, detoxifies, and protects cells. Gamma-glutamyl transferase (GGT), a key liver function biomarker, indicates liver disease and chronic conditions like diabetes and cancer. GGT metabolizes glutathione (GSH), which defends against free radicals from poor diet, alcohol, tobacco, and medications. High GGT levels signal oxidative stress and tissue damage, worsened by toxins, hormonal imbalances, and genetics. Managing GGT through hydration, a plant-based diet, reduced medication, vitamins, and stress management improves health and reduces risks.
Source References and Supplemental Research
1. Levinson M, Holbert J, Blackwell C, Wruble LD. Serum gamma‑glutamyl transpeptidase: Its specificity and clinical value. South Med J 1979;72:837‑41.doi:10.1097/00007611-197907000-00021[PubMed]
2. Kasarala G, Tillmann HL. Standard liver tests. Clin Liver Dis (Hoboken). 2016;8(1):13-18. Published 2016 Jul 26. doi:10.1002/cld.562 [PubMed][CrossRef]
3. Whitfield JB. Gamma glutamyl transferase. Crit Rev Clin Lab Sci. 2001;38(4):263-355. doi:10.1080/20014091084227 [PubMed][Crossref]
4. Lee DH, Jacobs DR Jr. Association between serum gamma-glutamyltransferase and C-reactive protein. Atherosclerosis. 2005;178(2):327-330. doi:10.1016/j.atherosclerosis.2004.08.027 [PubMed] [Crossref]
5. Fraser A, Harris R, Sattar N, Ebrahim S, Smith GD, Lawlor DA. Gamma-glutamyltransferase is associated with incident vascular events independently of alcohol intake: analysis of the British Women’s Heart and Health Study and Meta-Analysis [published correction appears in Arterioscler Thromb Vasc Biol. 2008 Feb;28(2):e14]. Arterioscler Thromb Vasc Biol. 2007;27(12):2729-2735. doi:10.1161/ATVBAHA.107.152298 [PubMed][Crossref]
6. Lee DH, Ha MH, Kim JH, et al. Gamma-glutamyltransferase and diabetes–a 4 year follow-up study. Diabetologia. 2003;46(3):359-364. doi:10.1007/s00125-003-1036-5 [PubMed][Crossref]
7. Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med. 2002;137(1):1-10. doi:10.7326/0003-4819-137-1-200207020-00006 [PubMed][Crossref]
8.Terzyan SS, Burgett AW, Heroux A, Smith CA, Mooers BH, Hanigan MH. Human γ-Glutamyl Transpeptidase 1: Structures of the Free Enzyme, Inhibitor-Bound Tetrahedral Transition States, and Glutamate-Bound Enzyme Reveal Novel Movement Within the Active Site During Catalysis. J Biol Chem. 2015;290(28):17576-17586. doi:10.1074/jbc.M115.659680 [PDB]
9. Zhang H, Forman HJ, Choi J. Gamma-glutamyl transpeptidase in glutathione biosynthesis. Methods Enzymol. 2005;401:468-483. doi:10.1016/S0076-6879(05)01028-1 [PubMed][Crossref]
10. Bai C, Zhang M, Zhang Y, He Y, Dou H, Wang Z, Wang Z, Li Z, Zhang L. Gamma-Glutamyltransferase Activity (GGT) Is a Long-Sought Biomarker of Redox Status in Blood Circulation: A Retrospective Clinical Study of 44 Types of Human Diseases. Oxidative Medicine and Cellular Longevity. 2005. [Crossref]
11. Siegel R, Miller K, Wagle N, Jemal A. Cancer Statistics, 2023. CA: A Cancer Journal for Clinicians. 2023; 73(1): 17-48. https://doi.org/10.3322/caac.21763. [Crossref]
12. Lee YJ, Han KD, Kim DH, Lee CH. Determining the association between repeatedly elevated serum gamma-glutamyltransferase levels and risk of respiratory cancer: A nationwide population-based cohort study. Cancer Med. 2021;10(4):1366-1376. doi:10.1002/cam4.3735 [PubMed]
13. Hong SW, Lee HJ, Han K, et al. Risk of gastrointestinal cancer in patients with an elevated level of gamma-glutamyltransferase: A nationwide population-based study. PLoS One. 2021;16(2):e0245052. Published 2021 Feb 5. doi:10.1371/journal.pone.0245052 [PubMed]
14. Hayes JD, Flanagan JU, Jowsey IR. Glutathione transferases. Annu Rev Pharmacol Toxicol. 2005;45:51-88. doi:10.1146/annurev.pharmtox.45.120403.095857 [PubMed]
15. Lushchak VI. Glutathione homeostasis and functions: potential targets for medical interventions. J Amino Acids. 2020;2020:1-18 [PubMed]
16. Marí M, Morales A, Colell A, García-Ruiz C, Fernández-Checa JC. Mitochondrial glutathione, a key survival antioxidant. Antioxid Redox Signal. 2009;11(11):2685-2700. doi:10.1089/ARS.2009.2695 [PubMed]
17. Ravasi G, Pelucchi S, Greni F, et al. Circulating factors are involved in hypoxia-induced hepcidin suppression. Blood Cells Mol Dis. 2014;53(4):204-210. doi:10.1016/j.bcmd.2014.06.006 [PubMed]
18. Grant C. Role of the glutathione/glutaredoxin and thioredoxin systems in yeast growth and response to stress conditions. Molecular Microbiology. 2001;39(3): 533-541. https://doi.org/10.1046/j.1365-2958.2001.02283.x [Crossref]
19. Ha SB, Smith AP, Howden R, et al. Phytochelatin synthase genes from Arabidopsis and the yeast Schizosaccharomyces pombe. Plant Cell. 1999;11(6):1153-1164. doi:10.1105/tpc.11.6.1153 [PubMed]
20. Dringen R. Metabolism and functions of glutathione in brain. Progress in Neurobiology. 2000;62(6):649-671. PMID 10880854. doi:10.1016/s0301-0082(99)00060-x. [PubMed] [Elsevier]
21. Scholz RW, Graham KS, Gumpricht E, Reddy CC. Mechanism of interaction of vitamin E and glutathione in the protection against membrane lipid peroxidation. Annals of the New York Academy of Sciences. 1989;570 (1): 514-517.PMID 14223080. doi:10.1111/j.1749-6632.1989.tb14973.x. [Wiley]
22. Hughes RE.. Reduction of dehydroascorbic acid by animal tissues. Nature. 1964;203(4949):1068-1069. PMID 14223080. doi:10.1038/2031068a0. [nature]
23. Meister A. On the enzymology of amino acid transport. Science. 1973;180(4081):33-39. PMID: 4144403. doi: 10.1126/science.180.4081.33. [Science]
24. Grant CM (2001). “Role of the glutathione/glutaredoxin and thioredoxin systems in yeast growth and response to stress conditions”. Molecular Microbiology. 39 (3): 533–541.
doi:10.1046/j.1365-2958.2001.02283.x. S2CID 6467802 [Wiley]
25. Melideo, SL; Jackson, MR; Jorns, MS (22 July 2014). “Biosynthesis of a central intermediate in hydrogen sulfide metabolism by a novel human sulfurtransferase and its yeast ortholog”. Biochemistry. 53 (28): 4739–53. doi:10.1021/bi500650h. [PubMed]
26. Ha SB, Smith AP, Howden R, Dietrich WM, Bugg S, O’Connell MJ, Goldsbrough PB, Cobbett CS (June 1999). Phytochelatin synthase genes from Arabidopsis and the yeast Schizosaccharomyces pombe. The Plant Cell. 11 (6): 1153–1164. doi:10.1105/tpc.11.6.1153. JSTOR 3870806. [PubMed]
27. Pompella A, Visvikis A, Paolicchi A, De Tata V, Casini AF. Pompella A, Corti A. Editorial: the changing faces of glutathione, a cellular protagonist. Front Pharmacol. 2015;6:98. PMID: 26029106. doi: 10.3389/fphar.2015.00098. [PubMed] [Elsevier]
28. Maher TJ, Glaeser BS, Wurtman RJ. Diurnal variations in plasma concentrations of basic and neutral amino acids and in red cell concentrations of aspartate and glutamate: effects of dietary protein intake. Am J Clin Nutr. 1984;39(5):722-729. PMID: 6538743. doi: 10.1093/ajcn/39.5.722.[PubMed]
29. Sies H (1999). “Glutathione and its role in cellular functions”. Free Radical Biology & Medicine. 27 (9–10): 916–921. doi:10.1016/S0891-5849(99)00177-X. [PubMed] [CrossRef]
30. Chen Y, Yang Y, Miller ML, Shen D, Shertzer HG, Stringer KF, Wang B, Schneider SN, Nebert DW, Dalton TP (May 2007). “Hepatocyte-specific Gclc deletion leads to rapid onset of steatosis with mitochondrial injury and liver failure”. Hepatology. 45 (5): 1118–1128. doi:10.1002/hep.21635. [Hepatology]
31. Hanigan MH. Gamma-glutamyl transpeptidase: redox regulation and drug resistance. Adv Cancer Res. 2014;122:103-141. doi:10.1016/B978-0-12-420117-0.00003-7 [PubMed]
32. West MB, Wickham S, Quinalty LM, Pavlovicz RE, Li C, Hanigan MH. Autocatalytic cleavage of human gamma-glutamyl transpeptidase is highly dependent on N-glycosylation at asparagine 95. J Biol Chem. 2011;286(33):28876-28888. doi:10.1074/jbc.M111.248823 [PubMed][CrossRef]
33. Kunutsor SK. Gamma-glutamyltransferase—friend or foe within? Liver International. 2016; 36(12); 1723-1734 https://doi.org/10.1111/liv.13221. [Wiley]
34. White CC, Viernes H, Krejsa CM, Botta D, Kavanagh TJ (July 2003). “Fluorescence-based microtiter plate assay for glutamate-cysteine ligase activity”. Analytical Biochemistry. 318 (2): 175–180. doi:10.1016/S0003-2697(03)00143-X. [Publication]
35. Guoyao Wu; Yun-Zhong Fang; Sheng Yang; Joanne R. Lupton; Nancy D. Turner (2004). “Glutathione Metabolism and its Implications for Health”. Journal of Nutrition. 134 (3): 489–492. doi:10.1093/jn/134.3.489. [PubMed] [Crossref]
36. Takemura K, Board PG, Koga F. A Systematic Review of Serum γ-Glutamyltransferase as a Prognostic Biomarker in Patients with Genitourinary Cancer. Antioxidants (Basel). 2021;10(4):549. Published 2021 Apr 1. doi:10.3390/antiox10040549 [PubMed]
37. Kamat PK, Mallonee CJ, George AK, Tyagi SC, Tyagi N. Homocysteine, Alcoholism, and Its Potential Epigenetic Mechanism. Alcohol Clin Exp Res. 2016;40(12):2474-2481. doi:10.1111/acer.13234 [PubMed]
38. Krajcovicová-Kudlácková, M., Blazícek, P., Kopcová, J., Béderová, A., & Babinská, K. (2000). Homocysteine levels in vegetarians versus omnivores. Annals of nutrition & metabolism, 44(3), 135–138. https://doi.org/10.1159/000012827 [PubMed] [Karger]
39. Esse, R.; Barroso, M.; Almeida, I.; Castro, R. The contribution of homocysteine metabolism disruption to endothelial dysfunction: State-of-the-art. Int. J. Mol. Sci. 2019, 20, 867. [Google Scholar] [CrossRef]
40. Azzini E, Ruggeri S, Polito A. Homocysteine: Its Possible Emerging Role in At-Risk Population Groups. International Journal of Molecular Sciences. 2020; 21(4):1421. https://doi.org/10.3390/ijms21041421 [MDPI]
41. Cleveland Clinic. Gamma-Glutamyl Transferase (GGT) Test. https://my.clevelandclinic.org/health/diagnostics/22055-gamma-glutamyl-transferase-ggt-test
42. Rosolová, H., Simon, J., Mayer, O., Jr, Racek, J., Dierzé, T., & Jacobsen, D. W. (2002). Unexpected inverse relationship between insulin resistance and serum homocysteine in healthy subjects. Physiological research, 51(1), 93–98. [PubMed] [Physiological Research]
43. Chiang EPI, Wang YC, Chen WW, Tang FY. Effects of Insulin and Glucose on Cellular Metabolic Fluxes in Homocysteine Transsulfuration, Remethylation,S-Adenosylmethionine Synthesis, and Global Deoxyribonucleic Acid Methylation. The Journal of Clinical Endocrinology & Metabolism. 2009;94(3):1017-1025. doi:https://doi.org/10.1210/jc.2008-2038 [Research Gate]
44. Stipanuk MH. Sulfur amino acid metabolism: pathways for production and removal of homocysteine and cysteine. Annu Rev Nutr. 2004;24:539-577. doi:10.1146/annurev.nutr.24.012003.132418. [PubMed]
45. Yorke E. Hyperthyroidism and Liver Dysfunction: A Review of a Common Comorbidity. Clin Med Insights Endocrinol Diabetes. 2022;15:11795514221074672. Published 2022 Feb 7. doi:10.1177/11795514221074672 [PubMed]
46. Bruinstroop E, van der Spek AH, Boelen A. Role of hepatic deiodinases in thyroid hormone homeostasis and liver metabolism, inflammation, and fibrosis. Eur Thyroid J. 2023;12(3):e220211. Published 2023 Apr 13. doi:10.1530/ETJ-22-0211 [PubMed]
47. Slyepchenko A, Brunoni AR, McIntyre RS, Quevedo J, Carvalho AF. The Adverse Effects of Smoking on Health Outcomes in Bipolar Disorder: A Review and Synthesis of Biological Mechanisms. Current Molecular Medicine. 2016;16(2):187-205. doi:https://doi.org/10.2174/1566524016666160126144601 [Research Gate]
48. O’Callaghan, P., Meleady, R., Fitzgerald, T., Graham, I., & European COMAC group (2002). Smoking and plasma homocysteine. European heart journal. 23(20); 1580-1586.[PubMed] [OxfordAcademic]
49. Kamat, P. K., Mallonee, C. J., George, A. K., Tyagi, S. C., & Tyagi, N. (2016). Homocysteine, Alcoholism, and Its Potential Epigenetic Mechanism. Alcoholism, clinical and experimental research. 40(12); 2474–2481. https://doi.org/10.1111/acer.13234 [PubMed] [EuropePMC]
50. Døssing M, Arlien-Søborg P, Petersen L, Ranek L. Liver damage associated with occupational exposure to organic solvents in house painters. European Journal of Clinical Investigation. 1983; 13(2): 151-157. [CrossRef]
51. Malaguarnera G, Cataudella E, Giordano M, Nunnari G, Chisari G, Malaguarnera M. Toxic hepatitis in occupational exposure to solvents. World J Gastroenterol. 2012;18(22):2756-2766. doi:10.3748/wjg.v18.i22.2756[PubMed]
52. Choi J, Bae S, Lim H, et al. Mercury Exposure in Association With Decrease of Liver Function in Adults: A Longitudinal Study. J Prev Med Public Health. 2017;50(6):377-385. doi:10.3961/jpmph.17.099 [PubMed]
53. Genchi G, Sinicropi MS, Lauria G, Carocci A, Catalano A. The Effects of Cadmium Toxicity. Int J Environ Res Public Health. 2020;17(11):3782. Published 2020 May 26. doi:10.3390/ijerph17113782 [PubMed]
54. Desouza C, Keebler M, McNamara DB, Fonseca V. Drugs Affecting Homocysteine Metabolism. Drugs. 2002;62(4):605-616. doi:https://doi.org/10.2165/00003495-200262040-00005 [Springer]
55. Larrey D, Pageaux GP. Drug-induced acute liver failure. European Journal of Gastroenterology & Hepatology. 2005;17(2):141-143. doi:10.1097/00042737-200502000-00002 [PubMed] [Crosslink]
56. Fontana RJ, Hayashi PH, Gu J, et al. Idiosyncratic drug-induced liver injury is associated with substantial morbidity and mortality within 6 months from onset. Gastroenterology. 2014;147(1):96-108.e4. doi:10.1053/j.gastro.2014.03.045 [PMC Full Text] [PubMed] [Crosslink]
57. McGill MR, Jaeschke H. Metabolism and disposition of acetaminophen: recent advances in relation to hepatotoxicity and diagnosis. Pharm Res. 2013;30(9):2174-2187. doi:10.1007/s11095-013-1007-6 [PMC Full Text] [PubMed] [Crosslink]
58. McGill MR, Sharpe MR, Williams CD, Taha M, Curry SC, Jaeschke H. The mechanism underlying acetaminophen-induced hepatotoxicity in humans and mice involves mitochondrial damage and nuclear DNA fragmentation. The Journal of Clinical Investigation. 2012;122(4):1574-1583. doi:10.1172/JCI59755 [PMC Full Text] [PubMed] [Crosslink]
59. Watkins PB, Kaplowitz N, Slattery JT, et al. Aminotransferase elevations in healthy adults receiving 4 grams of acetaminophen daily: a randomized controlled trial. JAMA. 2006;296(1):87-93. doi:10.1001/jama.296.1.87 [PubMed] [Crosslink]
60. Yuan L, Kaplowitz N. Mechanisms of drug-induced liver injury. Clinical Liver Disease. 2013;17(4):507-vii. doi:10.1016/j.cld.2013.07.002 [PMC Full Text] [PubMed] [Crosslink]
61. Devarbhavi H, Raj S, Aradya V, Rangegowda V, Veeranna G, Singh R, Reddy V, Patil M. Drug‐induced liver injury associated with stevens‐Johnson syndrome/toxic epidermal necrolysis: Patient characteristics, causes, and outcome in 36 cases. Hepatology. 2016; 63(3): 993-999. [CrossRef]
62. Kaplowitz N. Idiosyncratic drug hepatotoxicity. Nature Reviews Drug Discovery. 2005;4(6):489-499. doi:10.1038/nrd1750 [PubMed] [Crosslink]
63. Kraus, J. P., Janosík, M., Kozich, V., Mandell, R., Shih, V., Sperandeo, M. P., Sebastio, G., de Franchis, R., Andria, G., Kluijtmans, L. A., Blom, H., Boers, G. H., Gordon, R. B., Kamoun, P., Tsai, M. Y., Kruger, W. D., Koch, H. G., Ohura, T., & Gaustadnes, M. (1999). Cystathionine beta-synthase mutations in homocystinuria. Human mutation, 13(5), 362–375.[PubMed] [Wiley]
64. Scalise V, Balia C, Cianchetti S, et al. Non enzymatic upregulation of tissue factor expression by gamma-glutamyl transferase in human peripheral blood mononuclear cells. Thrombosis Journal. 2016;14:45. Published 2016 Nov 4. doi:10.1186/s12959-016-0119-8 [PubMed]
65. Reddy, S., Ramsubeik, K., Vega, K. J., Federico, J., & Palacio, C. (2010). Do HbA1C Levels Correlate With Delayed Gastric Emptying in Diabetic Patients?. Journal of neurogastroenterology and motility, 16(4), 414–417. https://doi.org/10.5056/jnm.2010.16.4.414 [JNM]
66. Abumrad NA, Davidson NO. Role of the gut in lipid homeostasis. Physiological Reviews. 2012; 92:1061-1085 [PMC free article] [PubMed]
67. Wilson J.G., Lindquist J.H., Grambow S.C., Crook E.D., Maher J.F. Potential role of increased iron stores in diabetes. Am. J. Med. Sci. 2003;325:332–339. doi: 10.1097/00000441-200306000-00004. [PubMed] [CrossRef]
68. Tiedge M., Lortz S., Drinkgern J., Lenzen S. Relation between antioxidant enzyme gene expression and antioxidative defense status of insulin-producing cells. Diabetes. 1997;46:1733–1742. doi: 10.2337/diab.46.11.1733. [PubMed] [CrossRef]
69. Dludla P.V., Joubert E., Muller C.J.F., Louw J., Johnson R. Hyperglycemia-induced oxidative stress and heart disease-cardioprotective effects of rooibos flavonoids and phenylpyruvic acid-2-O-beta-D-glucoside. Nutrition & Metabolism. 2017;14:45. doi: 10.1186/s12986-017-0200-8. [PMC free article] [PubMed] [CrossRef] [Google Scholar].
70. Žiberna, L., Jenko-Pražnikar, Z., & Petelin, A. (2021). Serum Bilirubin Levels in Overweight and Obese Individuals: The Importance of Anti-Inflammatory and Antioxidant Responses. Antioxidants (Basel, Switzerland), 10(9), 1352. https://doi.org/10.3390/antiox10091352 [PubMed] [MDPI] [PubMed]
71. Song Y, Liu J, Zhao K, Gao L, Zhao J. Cholesterol-induced toxicity: An integrated view of the role of cholesterol in multiple diseases. Cell Metabolism. 2021;33(10):1911-1925. doi:10.1016/j.cmet.2021.09.001 [Elsevier]
72. Chen P, Poddar R, Tipa EV, et al. Homocysteine metabolism in cardiovascular cells and tissues: implications for hyperhomocysteinemia and cardiovascular disease. Advances in Enzyme Regulation. 1999:39:93-109. PMID: 10470368 DOI: 10.1016/s0065-2571(98)00029-6. [PubMed]
73. Abhijit Basu A, Dvorina N, Baldwin W, Mazumder B. High‐fat diet‐induced GAIT element‐mediated translational silencing of mRNAs encoding inflammatory proteins in macrophage protects against atherosclerosis. FASEB Journal. March 2020; 34(5). DOI:10.1096/fj.201903119R [PubMed]
74. Chen, L., Deng, H., Cui, H., Fang, J., Zuo, Z., Deng, J., Li, Y., Wang, X., & Zhao, L. (2017). Inflammatory responses and inflammation-associated diseases in organs. Oncotarget, 9(6), 7204–7218. https://doi.org/10.18632/oncotarget.23208 [Oncotarget]
75. Kaushansky K, Lichtman MA, Prchal J, et al. Williams Hematology. 9th ed. New York: McGraw-Hill; 2015.
76. Stocker R, Yamamoto Y, McDonagh AF, Glazer AN, Ames BN. Bilirubin is an antioxidant of possible physiological importance. Science. 1987;235(4792):1043-1046. doi:10.1126/science.3029864 [PubMed] [Crosslink]
77. Badminton M.N., Elder G.H. Molecular mechanisms of dominant expression in porphyria. Journal of Inherited Metabolic Disease. 2005;28:277–286. doi: 10.1007/s10545-005-8050-3. [PubMed] [CrossRef] [Google Scholar]
78. Cruzat V, Macedo Rogero M, Noel Keane K, Curi R, Newsholme P. Glutamine: Metabolism and Immune Function, Supplementation and Clinical Translation. Nutrients. 2018;10(11):1564. Published 2018 Oct 23. doi:10.3390/nu10111564 [PubMed]
79. Weiss N, Jalan R, Thabut D. Understanding hepatic encephalopathy. Intensive Care Medicine. 2017; 44: 231-234. [CrossRef]
80. Albrecht J, Jones EA. Hepatic encephalopathy: molecular mechanisms underlying the clinical syndrome [published correction appears in J Neurol Sci 2000 Jan 1;172(1):77]. J Neurol Sci. 1999;170(2):138-146. doi:10.1016/s0022-510x(99)00169-0 [PubMed][CrossRef]
81. Ahboucha S, Butterworth RF. Pathophysiology of hepatic encephalopathy: a new look at GABA from the molecular standpoint. Metab Brain Dis. 2004;19(3-4):331-343. doi:10.1023/b:mebr.0000043979.58915.41[PubMed]
82. Rudler M, Weiss N, Bouzbib C, Thabut D. Diagnosis and Management of Hepatic Encephalopathy. Clinics in Liver Disease. 2021; 25(2): 393-417. https://doi.org/10.1016/j.cld.2021.01.008 [Elsevier]
83. Setién-Suero E, Suárez-Pinilla M, Suárez-Pinilla P, Crespo-Facorro B, Ayesa-Arriola R. Homocysteine and cognition: A systematic review of 111 studies. Neurosci Biobehav.Rev. 2016:69:280-98. PMID: 27531233. doi:10.1016/j.neubiorev.2016.08.014. [PubMed] [Elsevier]
84. Schaffer A, Verdoia M, Cassetti E, et al. Relationship between homocysteine and coronary artery disease. Results from a large prospective cohort study. Thromb Res. 2014;134(2):288-293. doi:10.1016/j.thromres.2014.05.025 [PubMed] [Elsevier]
85. Perna AF, Ingrosso D. Atherosclerosis determinants in renal disease: how much is homocysteine involved?. Nephrol Dial Transplant. 2016;31(6):860-863. doi:10.1093/ndt/gfv409 [PubMed] [CrossRef]
86. Professional, C. C. M. (n.d.). Chronic kidney disease. Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/15096-chronic-kidney-disease [ClevelandClinic]
87. Irizarry MC, Gurol ME, Raju S, et al. Association of homocysteine with plasma amyloid beta protein in aging and neurodegenerative disease. Neurology. 2005;65(9):1402-8. PMID: 16275827. doi: 10.1212/01.wnl.0000183063.99107.5c. [PubMed] [Neurology]
88. Ho PI, Ashline D, Dhitavat S, et al. Folate deprivation induces neurodegeneration: roles of oxidative stress and increased homocysteine. Neurobiology of Disease. 2003;14(1):32-42. doi: 10.1016/s0969-9961(03)00070-6. [Elsevier]
89. Kruman II, Culmsee C, Chan SL, et al. Homocysteine elicits a DNA damage response in neurons that promotes apoptosis and hypersensitivity to excitotoxicity. Journal of Neuroscience. 2000;20:6920-6926. DOI: 10.1523/JNEUROSCI.20-18-06920.2000. [PubMed] [JNeurosci] [PubMed]
90. Fuentes-Albero M, Cauli O. Homocysteine Levels in Autism Spectrum Disorder: A Clinical Update. Endocr Metab Immune Disord Drug Targets. 2018;18:289-296. PMID: 29437021 DOI: 10.2174/1871530318666180213110815. [PubMed] [BenthamScience]
91. Mattson MP, Shea TB. Folate and homocysteine metabolism in neural plasticity and neurodegenerative disorders. Trends Neurosci. 2003;26:137-146. DOI: 10.1016/S0166-2236(03)00032-8.. [PubMed] [CellPress]
92. Rossignol DA, Frye RE. Evidence linking oxidative stress, mitochondrial dysfunction, and inflammation in the brain of individuals with autism. Front Physiol. 2014:5:150. PMID: 24795645. doi: 10.3389/fphys.2014.00150. [PubMed] [Frontiers] [PubMed]
93.Coucke E, Akbar H, Kahloon A, Lopez P. Biliary Obstruction. StatPearls [Internet] https://www.ncbi.nlm.nih.gov/books/NBK539698/
94. Bile Duct Obstruction. Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/bile-duct-obstruction
95. Ramsay DJ. Homeostatic control of water balance. In: Arnaud MJ, editor. Hydration Throughout Life. Montrouge: John Libbey Eurotext; 1998. pp. 9–18. [Google Scholar]
96. Maroto-Sánchez, B., Lopez-Torres, O., Valtueña, J., Benito, P. J., Palacios, G., Díaz-Martínez, Á. E., González-Lamuño, D., Zinellu, A., González-Gross, M., & Carru, C. (2019). Rehydration during exercise prevents the increase of homocysteine concentrations. Amino acids, 51(2), 193–204. https://doi.org/10.1007/s00726-018-2655-y [PubMed] [Springer]
97. Ko C, Sekijima J, Lee S. Biliary Sludge. Annals of Internal Medicine. 1999; 130(4) [CrossRef]
98. Srivastava A. Progressive familial intrahepatic cholestasis. J Clin Exp Hepatol. 2014;4(1):25-36. doi:10.1016/j.jceh.2013.10.005[PubMed]
99. Kennedy M, Crozier S. How much water you’re actually supposed to drink each day — and why 8 cups isn’t right for everyone. Business Insiders: Reviews. December 14, 2021. https://www.businessinsider.com/guides/health/diet-nutrition/how-much-water-should-i-drink
100. Cardin R, Piciocchi M, Martines D, Scribano L, Petracco M, Farinati F. Effects of coffee consumption in chronic hepatitis C: A randomized controlled trial. Liver, Pancreas and Biliary Tract. 2013; 45(6):499-504. DOI:https://doi.org/10.1016/j.dld.2012.10.021 [CrossRef]
101. Danielsson J, Kangastupa P, Laatikainen T, Aalto M, Niemelä O. Dose- and Gender-dependent Interactions between Coffee Consumption and Serum GGT Activity in Alcohol Consumers. Alcohol and Alcoholism. 2013; 48(3):303-307. [Crossref]
102. Koenig G, Seneff S. Gamma-Glutamyltransferase: A Predictive Biomarker of Cellular Antioxidant Inadequacy and Disease Risk. Dis Markers. 2015;2015:818570. doi:10.1155/2015/818570 [PubMed]\
103. Koenig G, Seneff S. Gamma-glutamyltransferase: A predictive biomarker of cellular antioxidant inadequacy and disease risk. Dis Markers. 2015:2015:818570. PMID: 26543300. doi: 10.1155/2015/818570. [PubMed] [Wiley] [PubMed]
104. De Chiara F, Ureta Checcllo C, Ramón Azcón J. High Protein Diet and Metabolic Plasticity in Non-Alcoholic Fatty Liver Disease: Myths and Truths. Nutrients. 2019;11(12):2985. Published 2019 Dec 6. doi:10.3390/nu11122985 [PubMed]
105. Ho, P.I.; Ortiz, D.; Rogers, E.; Shea, T.B. Multiple aspects of homocysteine neurotoxicity: Glutamate excitotoxicity, kinase hyperactivation and DNA damage. J. Neurosci. Res. 2002, 70, 694–702. [Google Scholar] [CrossRef] [PubMed]
106. Moll S, Varga EA. Homocysteine and MTHFR Mutations. Circulation. 2015;132(1). doi:https://doi.org/10.1161/circulationaha.114.013311 [AHA Journals]
107. Krishnaswamy K, Lakshmi AV. Role of nutritional supplementation in reducing the levels of homocysteine. J Assoc Physicians India. 2002;50 Suppl:36-42. [PubMed]
108. Yi J, Thomas LM, Musayev FN, Safo MK, Richter-Addo GB. Crystallographic trapping of heme loss intermediates during the nitrite-induced degradation of human hemoglobin. Biochemistry. 2011;50(39):8323-8332. doi:10.1021/bi2009322 [ACS]
109. Hubbard SR, Hendrickson WA, Lambright DG, Boxer SG. X-ray crystal structure of a recombinant human myoglobin mutant at 2.8 A resolution. J Mol Biol. 1990;213(2):215-218. doi:10.1016/S0022-2836(05)80181-0 [PubMed] [Elsevier]
110. Rui L. Energy metabolism in the liver. Compr Physiol. 2014;4(1):177-197. doi:10.1002/cphy.c130024 [PubMed][CrossRef]
111. Consoli A, Nurjhan N, Capani F, Gerich J. Predominant role of gluconeogenesis in increased hepatic glucose production in NIDDM. Diabetes. 1989;38:550–557. [PubMed] [Google Scholar]
112. Magnusson I, Rothman DL, Katz LD, Shulman RG, Shulman GI. Increased rate of gluconeogenesis in type II diabetes mellitus. A 13C nuclear magnetic resonance study. J Clin Invest. 1992;90:1323–1327. [PMC free article] [PubMed] [Google Scholar]
113. Meyer C, Stumvoll M, Nadkarni V, Dostou J, Mitrakou A, Gerich J. Abnormal renal and hepatic glucose metabolism in type 2 diabetes mellitus. J Clin Invest. 1998;102:619–624. [PMC free article] [PubMed] [Google Scholar]
114. Send SR. Nutritional Management of Cholestasis. Clin Liver Dis (Hoboken). 2020;15(1):9-12. Published 2020 Feb 25. doi:10.1002/cld.865 [PubMed]
115. Zhang H, Tsao R. Dietary polyphenols, oxidative stress and antioxidant and anti-inflammatory effects. Current Opinion in Food Science. 2016;8:33-42. doi:10.1016/j.cofs.2016.02.002 [Elsevier]
116. Hurrell R, Egli I. Iron bioavailability and dietary reference values. Am J Clin Nutr. 2010;91(5):1461S-1467S. doi: 10.3945/ajcn.2010.28674F [PubMed] [Elsevier]
117. Cory, H., Passarelli, S., Szeto, J., Tamez, M., & Mattei, J. (2018). The Role of Polyphenols in Human Health and Food Systems: A Mini-Review. Frontiers in nutrition, 5, 87. https://doi.org/10.3389/fnut.2018.00087 [PubMed]
118. Desai A, Sequeira JM, Quadros EV. The metabolic basis for developmental disorders due to defective folate transport. Biochimie. 2016;126:31-42. doi:10.1016/j.biochi.2016.02.012 [PubMed] [Elsevier]
119. Savage K, Porter C, Bunnett E, Hana M, Keegan A, Ogden E, Stough C, Pipingas A. Liver and inflammatory biomarker relationships to depression symptoms in healthy older adults. Experimental Gerontology. 2023 https://doi.org/10.1016/j.exger.2023.112186. [Crossref]
120. Deminice R, Ribeiro DF, Frajacomo FT. The Effects of Acute Exercise and Exercise Training on Plasma Homocysteine: A Meta-Analysis. PLoS One. 2016;11(3):e0151653. Published 2016 Mar 17. doi:10.1371/journal.pone.0151653 [PubMed]
121. Ranjbar M, Shab-Bidar S, Mohammadi H, Djafarian K. Effect of Intermittent Fasting on Liver Function Tests: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Nutrition Reviews. 2024. https://doi.org/10.1093/nutrit/nuae070. [CrossRef]
122. Li X, Fan S, Cai C, et al. YAP regulates the liver size during the fasting-refeeding transition in mice. Acta Pharm Sin B. 2023;13(4):1588-1599. doi:10.1016/j.apsb.2022.12.011 [PubMed]
123. Mehrabani S, Bagherniya M, Askari G, Read MI, Sahebkar A. The effect of fasting or calorie restriction on mitophagy induction: a literature review. J Cachexia Sarcopenia Muscle. 2020;11(6):1447-1458. doi:10.1002/jcsm.12611 [PubMed]
124. Scommegna P, Mather M. Up to Half of U.S Premature Deaths Are Preventable; Behavioral Factors Key. Published September 14, 2015. https://www.prb.org/resources/up-to-half-of-u-s-premature-deaths-are-preventable-behavioral-factors-key/
125. Zhang Z, Ma L, Geng H, Bian Y. Effects of Smoking, and Drinking on Serum Gamma-Glutamyl Transferase Levels Using Physical Examination Data: A Cross-Sectional Study in Northwest China. Int J Gen Med. 2021;14:1301-1309. Published 2021 Apr 15. doi:10.2147/IJGM.S301900 [PubMed]
126. Harvard T.H Chan School of Public Health Antioxidants. The Nutrition Source. https://nutritionsource.hsph.harvard.edu/antioxidants/
127. Casas-Grajales S, Muriel P. Antioxidants in liver health. World J Gastrointest Pharmacol Ther. 2015;6(3):59-72. doi:10.4292/wjgpt.v6.i3.59 [PubMed]
128. Ghasemian M, Owlia S, Owlia MB. Review of Anti-Inflammatory Herbal Medicines. Adv Pharmacol Sci. 2016;2016:9130979. doi:10.1155/2016/9130979 [PubMed]
129. Li J, Cordero P, Nguyen V, Oben JA. The Role of Vitamins in the Pathogenesis of Non-alcoholic Fatty Liver Disease. Integr Med Insights. 2016;11:19-25. Published 2016 Apr 27. doi:10.4137/IMI.S31451[PubMed]
130. Gusdon A, Song K, Qu S. Nonalcoholic Fatty Liver Disease: Pathogenesis and Therapeutics from a Mitochondria-Centric Perspective. Oxidative Medicine and Cellular Longevity. 2014. https://doi.org/10.1155/2014/637027 [Wiley]
131. Harvard T.H Chan School of Public Health Antioxidants. Niacin- Vitamin B3. https://nutritionsource.hsph.harvard.edu/niacin-vitamin-b3/
132. McRae MP. Betaine supplementation decreases plasma homocysteine in healthy adult participants: a meta-analysis. J Chiropr Med. 2013;12(1):20-25. doi:10.1016/j.jcm.2012.11.001 [PubMed][CrossRef]
133. National Institutes of Health. Office of Dietary Supplements – Folate. Nih.gov. Published November 30, 2022. https://ods.od.nih.gov/factsheets/Folate-HealthProfessional/ [National Institutes of Health]
134. Hanna M, Jaqua E, Nguyen V, Clay J. B Vitamins: Functions and Uses in Medicine. Perm J. 2022;26(2):89-97. doi:10.7812/TPP/21.204 [PubMed] [PMC Full Text] [Crosslink]
135. Nagasawa, Herbert T. (27 November 2014). “Compositions comprising sugar-cysteine products – US-20140348811-A1”. ppubs.uspto.gov. United States Patent Office. p. 16. Retrieved 31 October 2023. 30. A method of increasing ATP and/or glutathione.”
136. Ukwenya VO, Alese MO, Ogunlade B, Folorunso IM, Omotuyi OI. Anacardium occidentale leaves extract and riboceine mitigate hyperglycemia through anti-oxidative effects and modulation of some selected genes associated with diabetes. J Diabetes Metab Disord. 2022;22(1):455-468. Published 2022 Dec 8. doi:10.1007/s40200-022-01165-2 [PubMed][CrossRef]
137. Betaine Information | Mount Sinai – New York. Mount Sinai Health System. Accessed July 29, 2024. [Mount Sinai]
138. Betaine (Oral Route) Proper Use – Mayo Clinic. www.mayoclinic.org. Accessed July 29, 2024. [Mayo Clinic]
139. Olthof MR, van Vliet T, Boelsma E, Verhoef P. Low dose betaine supplementation leads to immediate and long term lowering of plasma homocysteine in healthy men and women. J Nutr. 2003;133(12):4135-4138. doi:10.1093/jn/133.12.4135 [PubMed]