Homocysteine: Diagnostic Significance and Clinical Insights
Authors: Dr. Payal Bhandari, M.D., Hailey Chin
Contributors: Vivi Chador, Amer Džanković, Nigella Umali Ruguian
Key Insights
Homocysteine (Hcy) is an amino acid made when the body breaks down methionine, found in protein-rich foods. Hcy helps recycle molecules and build proteins. Methionine is converted to S-adenosyl-L-methionine (SAMe), which helps make hormones and other chemicals. SAMe turns into -Adenosyl-L-Homocysteine (SAH), which becomes Hcy. With enough B vitamins (B6, B9, B12), Hcy either turns back into methionine or becomes cysteine. High Hcy levels can signal problems with protein breakdown or B vitamin deficiencies. Low Hcy might mean too many B vitamins or fast conversion to cysteine, lowering glutathione (GSH), an important antioxidant. Measuring Hcy and B vitamin levels can help identify health issues, guide diet and supplements, and improve treatment for chronic conditions.
What is Homocysteine?
Definition of Homocysteine
Homocysteine (Hcy) is made when the body breaks down dietary protein. It helps recycle molecules, build new proteins, and support metabolism. Vitamins B6, B9, and B12 help keep Hcy levels low in the blood.
Physiology of Homocysteine1
Homocysteine (Hcy) is made when the body breaks down methionine, an amino acid in protein-rich foods. Methionine contains sulfur and helps create other essential amino acids.
Amino Acids are the Building Blocks of Protein
Proteins are made of amino acids, the building blocks of life. Each amino acid has an amino group (-NH2), carboxyl group (-COOH), and unique side chain (R). Of the 20 amino acids essential for protein synthesis, some must be obtained from food. Amino acids link via peptide bonds into chains, with their sequence determining protein shape and function. Even minor changes can impact function, causing diseases or enhancing activity.
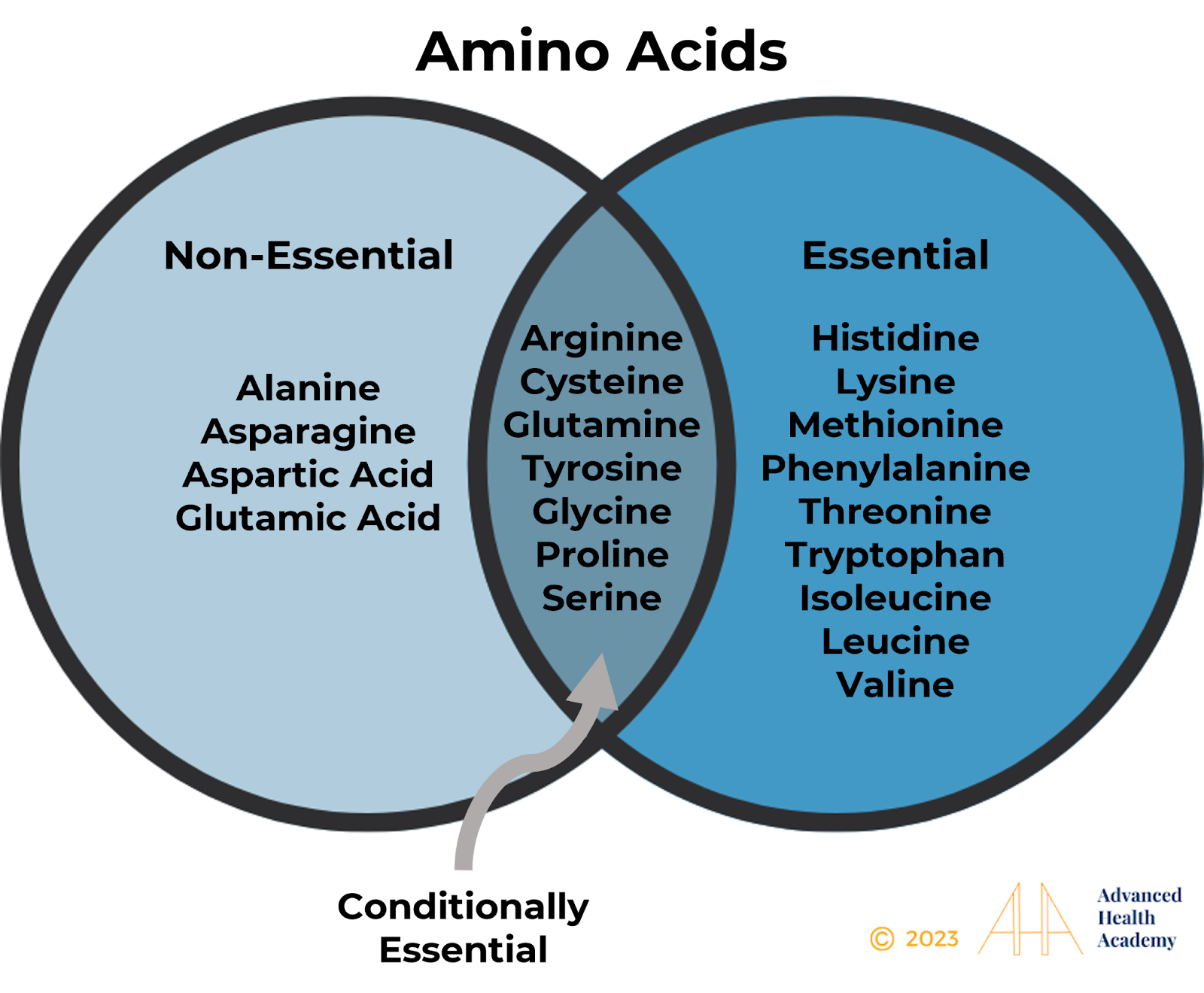
Figures 1: Essential and Non-Essential Amino Acids
Protein Metabolism and Synthesis in the Body
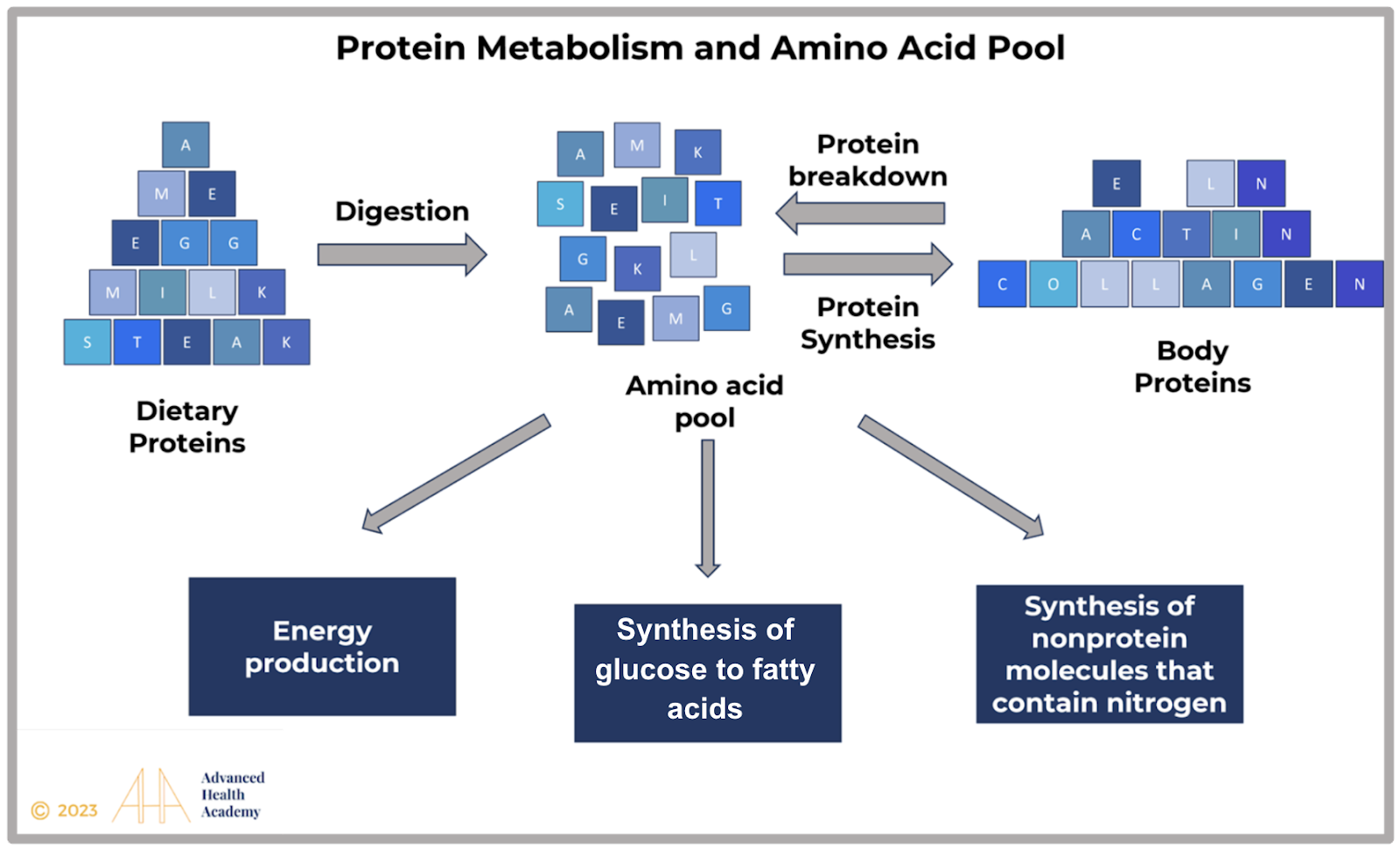
Figure 2: Protein cannot be stored and is broken into amino acids for new proteins, nonessential amino acids, and nitrogen compounds. Excess protein converts to glycogen or fat for energy or metabolic pathways.
Formation of Homocysteine
Homocysteine (Hcy) forms in the body after eating foods high in methionine, like meat, nuts, and oils. Here’s the process:
Methionine Activation: Methionine gets an energy group from ATP.
Methyl Group Transfer: Enzymes add a methyl group to methionine, forming SAMe, which donates the group to DNA, RNA, and proteins, turning into SAH.
SAH Breakdown: An enzyme splits SAH into adenosine and Hcy.
Hcy Circulation: Most Hcy binds to albumin in the blood, with 99% reabsorbed by the kidneys and 1% excreted in urine.
Remethylation: Hcy turns back into methionine with folate, MTHFR, and vitamin B12.
Transsulfuration: Hcy combines with serine to form cystathionine, helped by vitamin B6, which breaks down into cysteine for making antioxidants like glutathione.
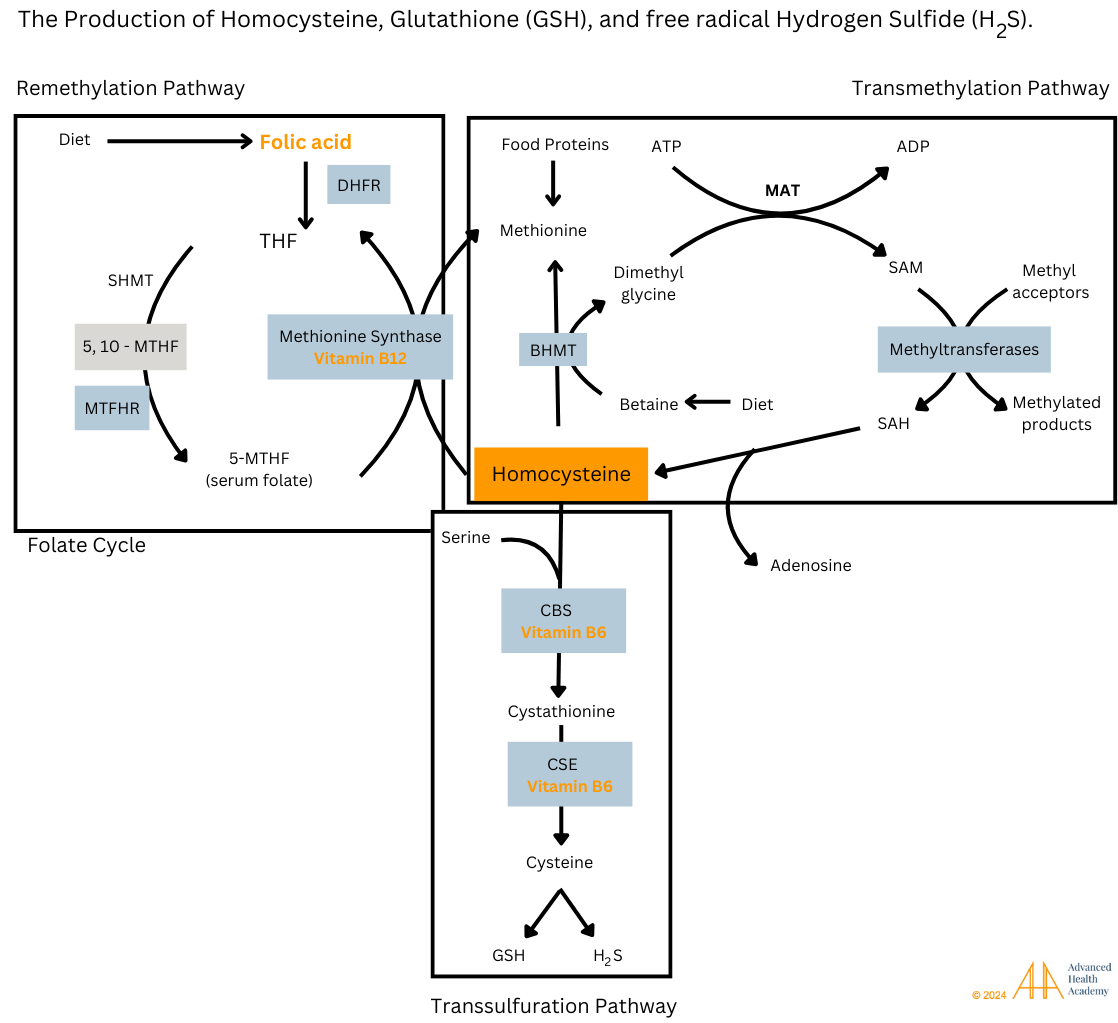
Figure 3: Homocysteine (Hcy) follows two pathways in cells: one turns it into methionine, and the other into cystathionine. These processes are controlled by SAM and SAH, which depend on vitamins B6, B9, and B12. SAM and SAH help make important molecules like creatine, detoxify the body, produce energy (ATP), and support neurotransmitters.
(DHFR = dihydrofolate reductase; THF = tetrahydrofolate; SHMT = serine hydroxymethyltransferase; MTHF = methylenetetrahydrofolate; MTHFR = 5,10-methylene-THF reductase; ATP = adenosine triphosphate; MAT = methionine adenosyltransferase; ADP = adenosine diphosphate; SAM = S-adenosylmethionine; SAH = S-adenosylHcy; BHMT = betaine-Hcy S-methyltransferase; CBS = cystathionine β-synthase; CSE = cystathionase; GSH = glutathione; H2S = hydrogen sulfide).
Role of Homocysteine in the Body
Homocysteine stores cysteine, which is used to produce glutathione (GSH), a powerful antioxidant. GSH has key roles in the body:
Protects cells, especially mitochondria, from damage by harmful molecules like ROS and inflammation.
Supports liver detox by helping remove harmful substances.
Eliminates toxins, including ROS and peroxides.
Aids in immune responses and controls inflammation.
Keeps vitamins C and E active as antioxidants.
Helps repair DNA, proteins, and other cell parts.
Supports brain function and mood regulation.
Boosts immune and nerve cell health.
Transports amino acids for cell health and longevity.
Low levels of GSH are linked to aging and conditions like cancer, heart disease, and neurodegenerative disorders.
Regulation of Homocysteine
Homocysteine (Hcy) levels are influenced by hormones, diet, and medications. Vitamins B6, B9, and B12, found in dark green veggies, legumes, and whole grains like quinoa, wheat, oats, and brown rice, help control Hcy levels and reduce the risk of tissue damage from high Hcy and oxidative stress.
Hormonal Regulation
Insulin helps lower homocysteine (Hcy) by turning it into methionine, which reduces cysteine and glutathione (GSH) production. It also supports fat metabolism and energy (ATP), which are important for DNA, RNA, and cell repair while keeping harmful ROS low. When insulin is low, blood sugar rises, Hcy levels increase, cysteine drops, and ATP production slows, causing more ROS and cell damage.
Cortisol, a stress hormone, raises Hcy by breaking down proteins or turning food into glucose. This releases Hcy-building blocks. High cortisol from stress also increases ROS, which damages cells. Vitamin C can lower both Hcy and cortisol levels, reducing stress on the adrenal glands.
Diet
Your diet affects the levels of proteins and amino acids in your blood, which impacts your health. For example, methionine (Met), found in meat, nuts, and legumes, can raise homocysteine (Hcy) levels if eaten in excess. High Hcy is linked to health problems. Eating foods rich in B6 and B9 (like dark green vegetables) helps lower Hcy by supporting key body processes. Polyphenols in foods like tea, coffee, berries, and fermented items can reduce nutrient absorption (e.g., iron and zinc). While polyphenols protect cells and support gut health, too many can interfere with nutrient processing. Eating too much methionine or polyphenol-rich foods can raise Hcy levels, lower antioxidants like glutathione, and harm blood health over time.
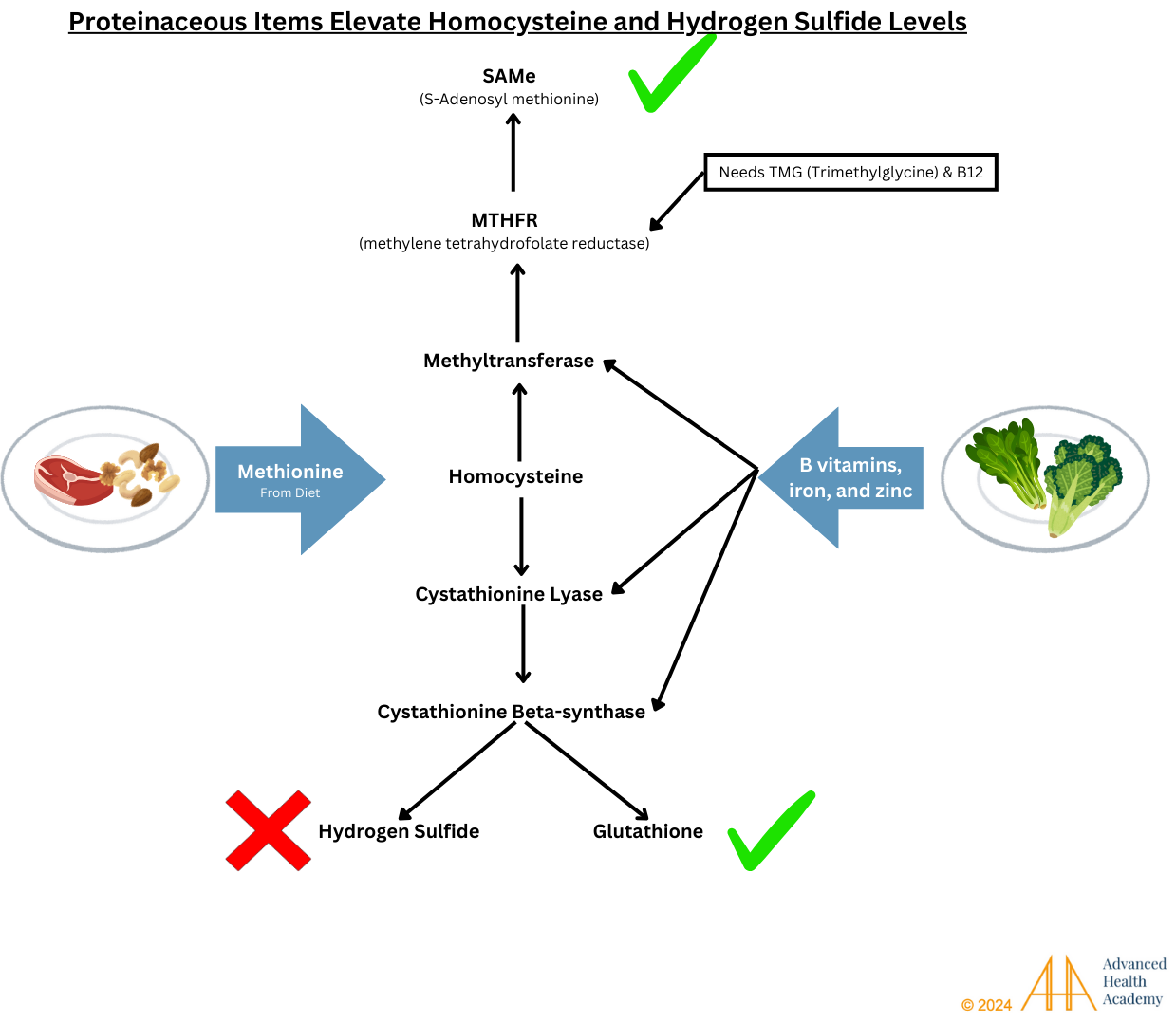
Figure 4: Eating too much protein from animal products and nuts can stop the body from properly recycling homocysteine (Hcy), raising Hcy levels. A lack of B vitamins, found in green vegetables and a healthy gut, can change the MTHFR enzyme gene, disrupting important body processes. This leads to a faster breakdown of glutathione (GSH), a key antioxidant. The enzyme GGT and hydrogen sulfide (H2S) speed up cell damage, harming organs and tissues.
Drugs
Smoking reduces blood flow, increases cortisol, and raises blood sugar, which creates harmful proteins like TNF-alpha, interleukins, and reactive oxygen species (ROS). The cadmium in nicotine lowers the effectiveness of antioxidants like vitamins C and E, and glutathione, and reduces hormone production, including serotonin and melatonin.
Alcohol and its breakdown products affect liver genes and DNA. Acetaldehyde, a byproduct of alcohol, disrupts the conversion of homocysteine to methionine, lowering cysteine and glutathione production and increasing homocysteine levels. Long-term alcohol use can damage the liver, cause inflammation and scarring, and lead to liver failure. Studies show that limiting alcohol intake helps maintain stable homocysteine levels and supports glutathione production.

Figure 5: Acetaldehyde, a byproduct of alcohol, disrupts the balance between SAM and SAH. This causes more homocysteine (Hcy) to turn into methionine, reducing cysteine and glutathione (GSH) production. Lower GSH levels increase the risk of tissue damage from oxidative stress and affect functions like making molecules and neurotransmitters, detoxifying and balancing hormones, and producing energy.
Pharmaceutical Medications
Long-term use of certain drugs can affect the body’s ability to absorb B vitamins and interfere with liver processes. Some drugs also use a lot of heme iron, which reduces iron and oxygen for other organs, possibly causing tissue damage and increasing harmful molecules.
Drug-induced liver injury (DILI) is a leading cause of acute liver failure and can be life-threatening. It is also a common reason for drugs to be withdrawn from the market. There are two types of DILI: intrinsic and idiosyncratic.
Intrinsic DILI happens in predictable patterns, such as taking over 7.5g of acetaminophen (APAP) in one dose, which can cause liver damage. Even the approved 4g/day dose for two weeks can raise liver enzyme levels in about a third of patients.
Idiosyncratic DILI (IDILI) is harder to predict and doesn’t depend on the dose. It can take weeks or months to develop and causes 10-15% of acute liver failure in the U.S. Factors like an unhealthy gut microbiome and blood vessel inflammation can increase the risk of drug reactions. Repeated drug use worsens liver damage, affecting protein and fat processing.
DILI can resemble a viral liver infection, but diagnosing it is difficult. Liver biopsies often don’t help, as symptoms are similar to other liver conditions. A higher number of eosinophils (white blood cells) is rare in DILI cases.

Figure 6: Drug-Induced Liver Injury. The accumulation and metabolism of drugs in the liver can cause a variety of pathophysiologic complications.
Clinical Significance of High Homocysteine Levels
Figure 7: Decoding Homocysteine’s Role in Health
Homocysteine (Hcy) is a useful marker for detecting health issues. High Hcy levels are linked to shorter lifespans. Deficiencies in vitamins B6, B9 (folate), or B12 lower antioxidant activity and increase harmful molecules like reactive oxygen species (ROS) and proinflammatory proteins. ROS can damage genes that produce blood cells, platelets, and metabolic proteins. For example, ROS can mutate the MTHFR gene, reducing Hcy conversion to methionine and raising Hcy levels. Mutations in the CBS gene also increase Hcy levels by affecting cystathionine conversion. Reduced cysteine storage raises gamma-glutamyl transferase (GGT) in the liver and kidneys, breaking down glutathione (GSH), an antioxidant. Lower GSH leads to faster tissue damage.
Atherosclerosis-Induced Vascular Inflammation
High homocysteine (Hcy) levels can lead to a number of health problems. In the bloodstream, low antioxidant levels make cholesterol more likely to oxidize, triggering a process called atherosclerosis. This narrows arteries, raises blood pressure, and causes damage to organs like the liver, heart, and pancreas.

Figure 8: Atherosclerosis causes artery thickening (tunica intima hyperplasia) and clot formation by platelets. Macrophages ingest oxidized LDL cholesterol, becoming foam cells that release inflammatory proteins and ROS. Chronic inflammation increases white blood cells and platelets, damaging cells and microbiota, reducing organ function, and raising the risk of health issues.
Liver Dysfunction and Damage
The liver’s role in processing fats, proteins, and balancing energy is disrupted by high Hcy, leading to fat buildup and inflammation. This can activate white blood cells (WBCs), causing more damage and reducing the body’s ability to fight off disease.
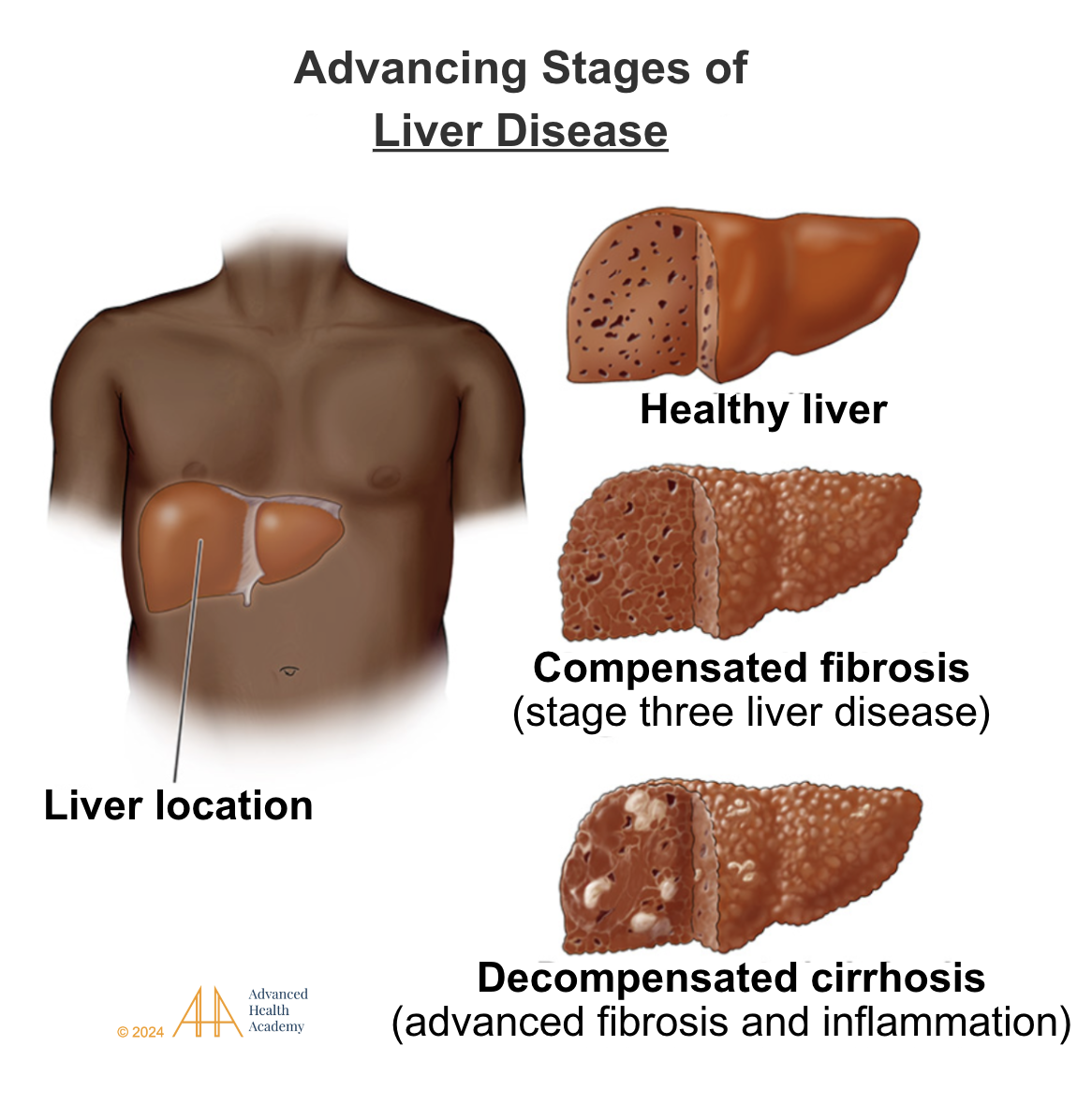
Figure 9: Chronic liver disease (steatosis, steatohepatitis, and cirrhosis, respectively, based on severity of progression) is associated with decreased harvesting of energy and increased production of reactive oxygen species (ROS). ROS mutate genes involved in various metabolic pathways throughout the body and prevent the detoxification and excretion of toxic waste.
Pancreatic Dysfunction and Damage
In the pancreas, Hcy can affect insulin and glucagon, leading to higher blood sugar, fat storage, and inflammation. This raises the risk of conditions like diabetes, atherosclerosis, and polycystic ovarian syndrome (PCOS). Symptoms of pancreatic issues include abdominal pain, weight gain, and digestive problems.
Kidney Dysfunction and Disease
High Hcy levels also impact the kidneys by breaking down glutathione, which harms kidney function. This can cause pain, swelling, and other kidney issues.
Bone Issues
In bones, high Hcy reduces blood flow, lowers bone mineral density, and increases the risk of osteoporosis and fractures. In the eyes, it can lead to retinopathy, optic nerve damage, and glaucoma by reducing blood flow and triggering inflammation.
Eye Issues
High homocysteine (Hcy) levels are linked to eye problems like retinopathy, optic nerve damage, and glaucoma. Hcy causes oxidative stress, reducing blood flow to the eyes and damaging eye cells, leading to inflammation, nerve damage, and faster cell death.
Brain and Nervous System Dysfunction and Damage
High Hcy levels interfere with SAMe and DNA methylation, affecting brain function. Hcy harms brain pathways and reduces important chemicals like serotonin, increasing the risk of brain damage and mental health issues.
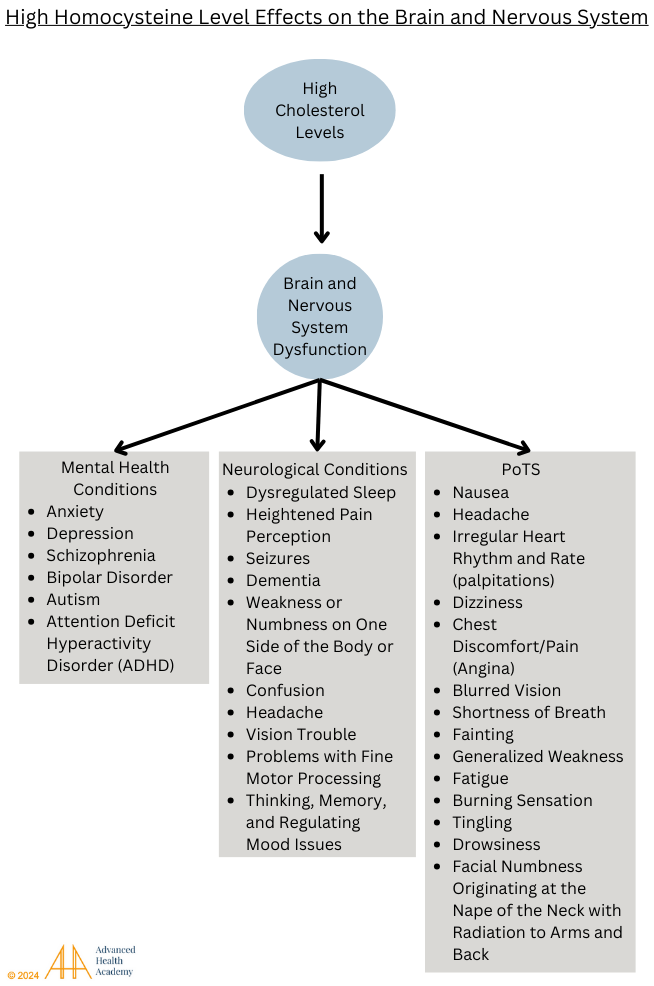
Figure 10: High homocysteine (HHcy) levels can damage multiple organs by producing toxic byproducts from cysteine and methionine. One common effect of HHcy is postural tachycardia syndrome (PoTS), which causes heart issues in people of all ages. PoTS is responsible for about 32.2% of fainting cases in children.
Cancer
Hcy competes with SAMe, affecting DNA methylation and harming brain function, which can lead to mental health and nervous system disorders. It also lowers glutathione levels, increasing oxidative stress and promoting cancer cell growth.
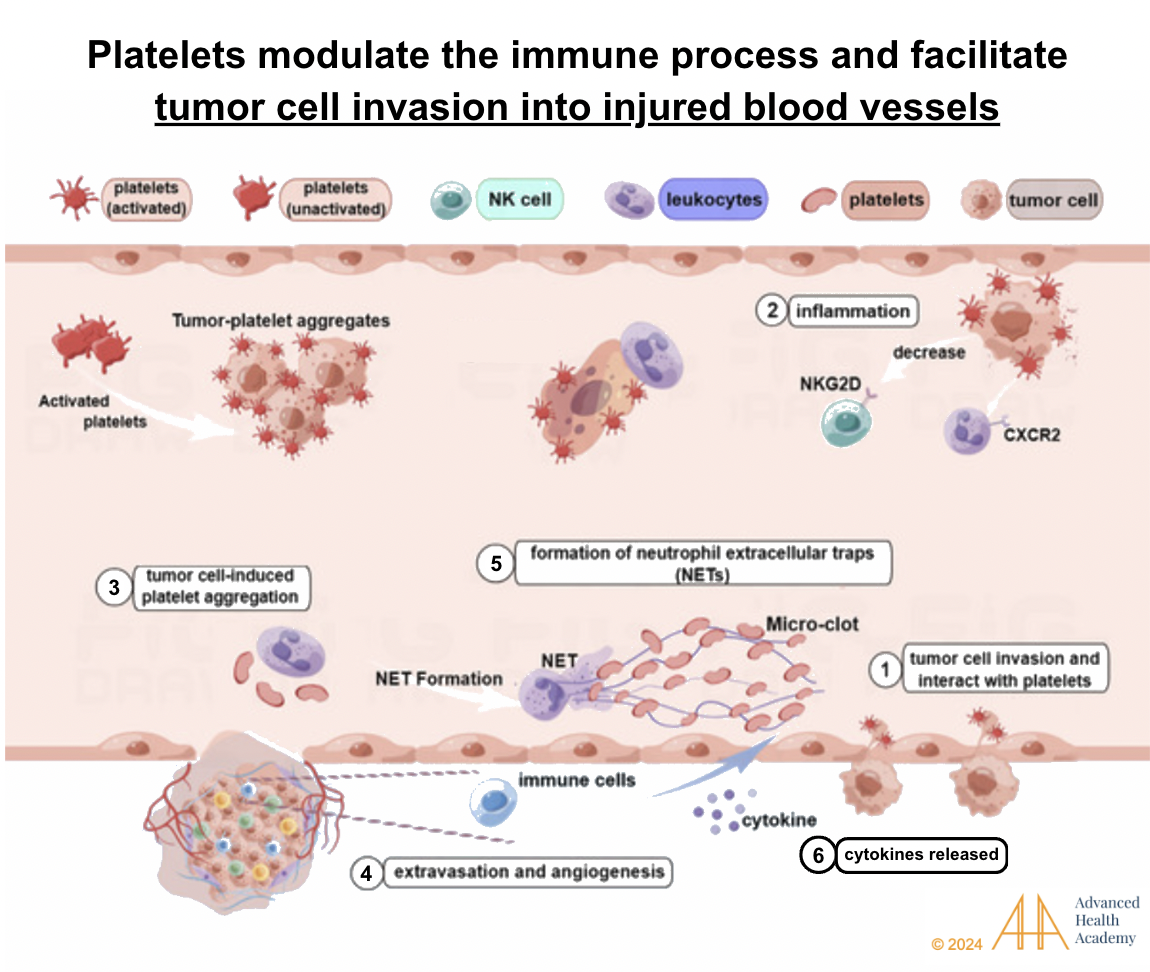
Figure 11: Platelets and tumor cells modulate the immune response and increase the production of proinflammatory proteins (like cytokines) and reactive oxygen species [inflammation] (1 and 2). Tumor cells induce platelet aggregation 64 (3) and support angiogenesis (new blood vessel formation) (4). Natural killer (NK) cells are prevented from ingesting and destroying tumor cells, pathogens, and other foreign invaders in circulation(5)54. Instead, neutrophils focus on assisting the stabilization and integrity of the blood vessel (2)64 and shielding tumor cells from destruction . Thus, the cytokines released from these reactions promote tumor growth, migration, and invasion into blood vessels (6) .
Adverse Pregnancy Outcomes
During pregnancy, high Hcy can cause complications like high blood pressure (e.g., preeclampsia), repeated miscarriages, birth defects, and premature birth. It can also affect hormone levels, kidney function, and glucose metabolism.
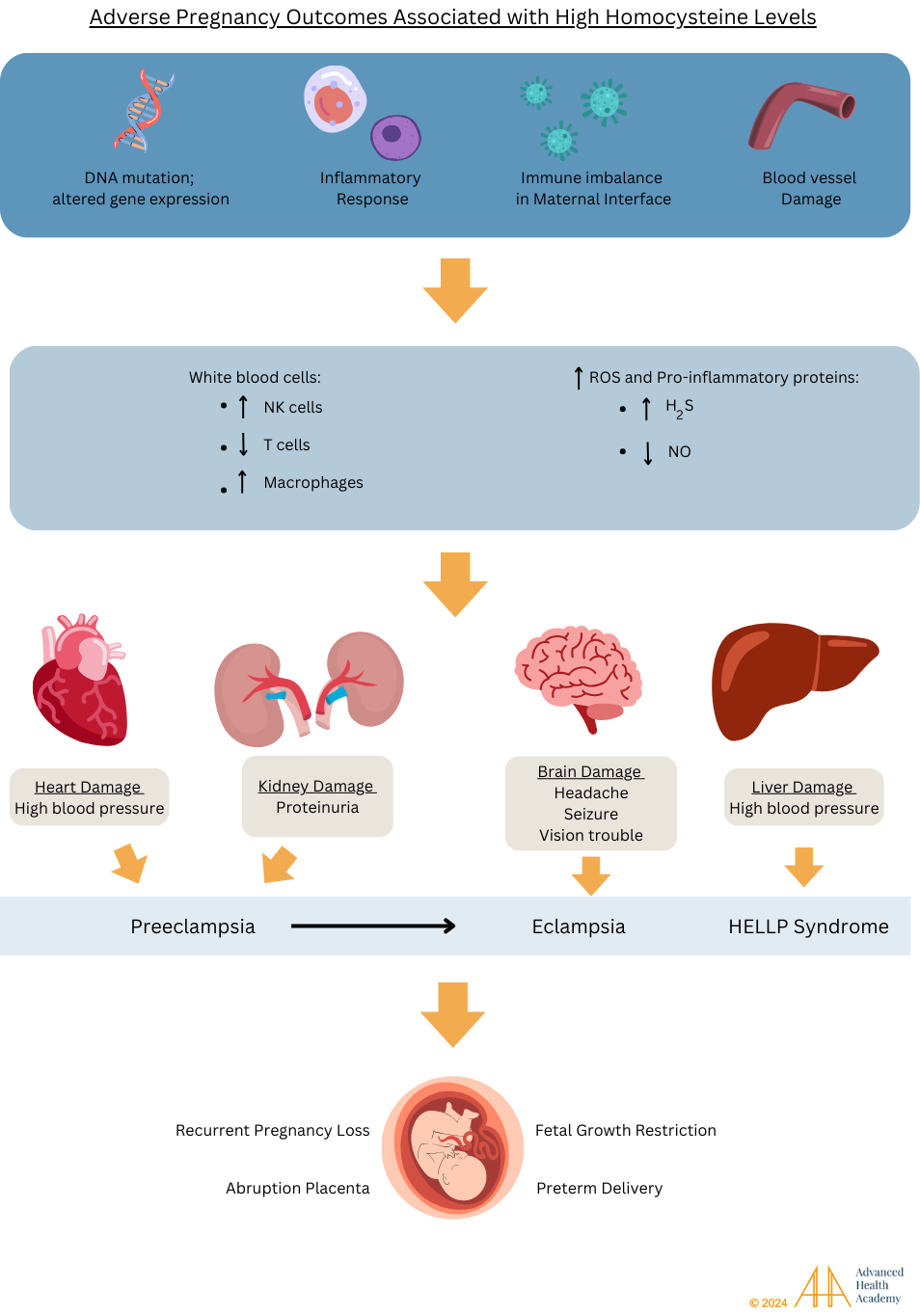
Figure 12: High homocysteine levels can lead to pregnancy problems by affecting enzymes and blood flow to the placenta. Vitamin deficiencies, DNA changes, and blood vessel damage harm the placenta, raising the risk of high blood pressure, preeclampsia, and other complications for mother and baby.
Clinical Significance of Low Homocysteine Levels
Low homocysteine (Hcy) levels usually indicate good health and enough vitamins B6, B9, and B12 from a balanced, plant-based diet. These vitamins help control Hcy levels. Low methionine intake (from animal products, nuts, and some legumes) or excess folate, B6, betaine, or N-acetylcysteine supplements can lower Hcy. During pregnancy, higher albumin levels can also reduce Hcy.
Hcy stores cysteine, which is needed to make glutathione (GSH), an important antioxidant. Too much methionine can lower both Hcy and GSH, leading to more free radicals and damage to DNA, RNA, and mitochondria. Mutations in the CBS gene can cause disorders like Down’s syndrome and peripheral neuropathy.
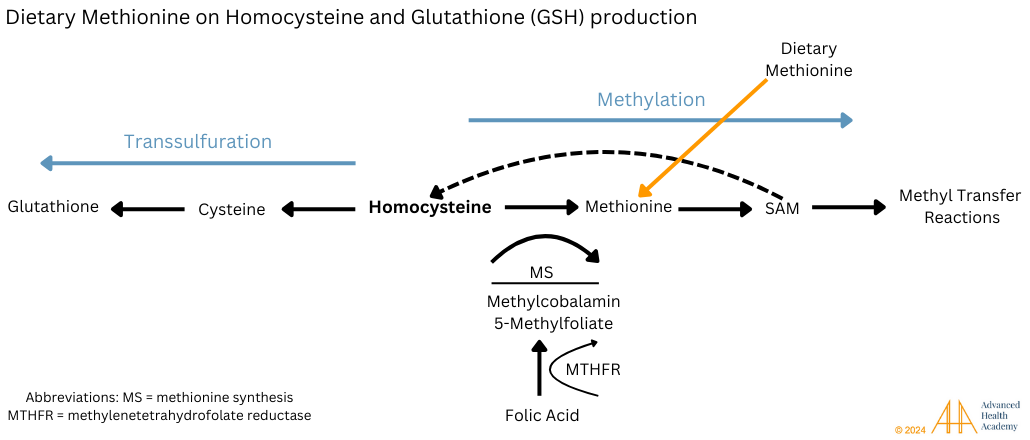
Figure 13: Dietary methionine increases the conversion of homocysteine (Hcy) to cysteine and, further to glutathione (GSH), resulting in low blood Hcy levels. GSH neutralizes free radicals, keeps oxidative stress under control, and prevents all-cause morbidity and mortality. Excess and chronic consumption of methionine-rich meals overutilizes this metabolic pathway, resulting in excess reactive oxygen species (ROS) production. ROS damages the genetic code of the enzymes involved in transmethylation and transsulfuration and increases the degradation of GSH and the free radical hydrogen sulfide (H2S) produced.
Prevalence and Statistics of Abnormal Homocysteine Levels
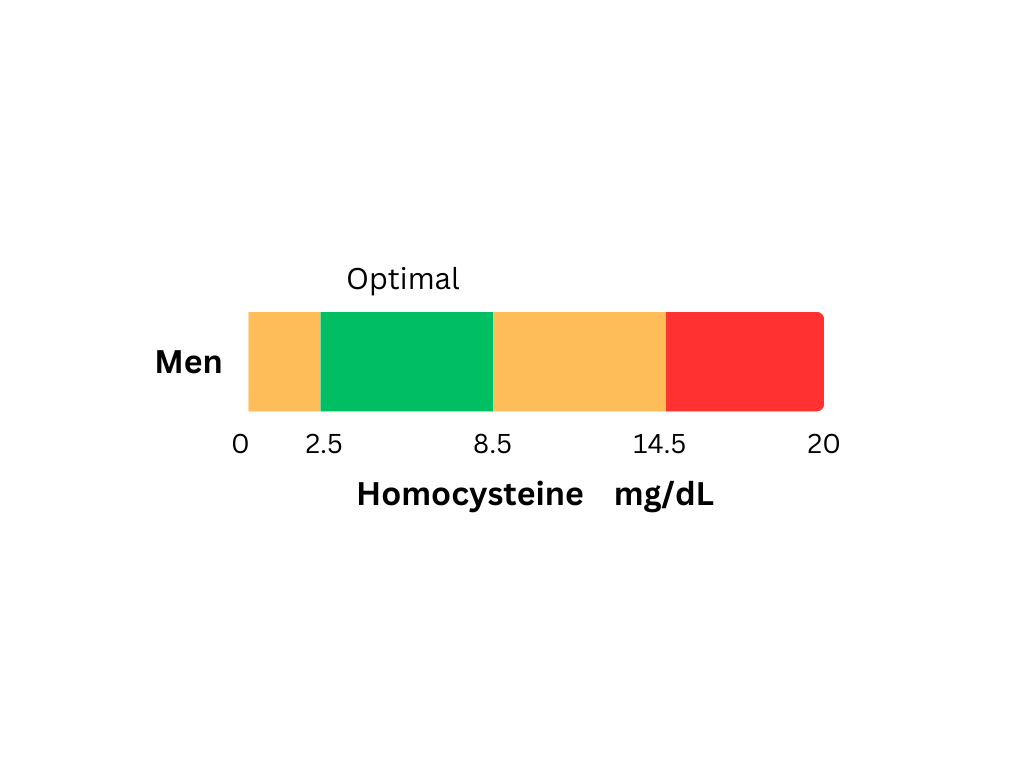
Both high and low homocysteine (Hcy) levels can signal health issues, particularly heart disease. High levels (over 15 micromol/L) and low levels (below 5 micromol/L) are affected by factors like diet, exercise, medications, age, sex, and health. For example, a larger waistline increases the risk of high Hcy by 5%, and smoking raises the risk by 24%. Eating fewer fruits and vegetables also increases the risk. A 5 μmol/L increase in Hcy raises the chance of early death by 33.6%.
High Hcy is often linked to low levels of vitamins B6, B9, and B12 and affects about 5% of people, with higher risks in those with poor diets, older adults, men, and people in low-income countries. In places like Ethiopia, high Hcy is linked to high blood pressure due to limited access to fresh produce. In India, 93% of men and 81% of women are affected.
Genetics can also cause high Hcy, with a common mutation in the MTHFR gene increasing the risk of heart disease and blood clots. Around 20-40% of white or Hispanic people carry this mutation, which reduces enzyme function by 35%. In some regions, 8-20% of people have a more severe form, reducing enzyme activity to just 30%.
Conclusion
Homocysteine (Hcy) is an important marker for checking metabolic health. High Hcy levels are often caused by low intake or poor metabolism of vitamins B6, B9, and B12 (found in green vegetables and citrus) or by gene mutations that affect Hcy breakdown. Low Hcy levels generally signal good health and proper metabolism in the body. Very low Hcy can happen with too much B vitamin supplementation or during pregnancy.
Tracking Hcy levels in lab tests can provide important information about a person’s risk for diseases and overall health. A healthy lifestyle with a balanced plant-based diet, staying hydrated, and regular exercise helps control Hcy levels and can reduce side effects from medications used for chronic conditions like diabetes, heart disease, and cancer. Research on how genetics, lifestyle, and diet affect Hcy metabolism can improve our understanding of how to prevent and manage chronic health issues.
Source References and Supplemental Research
Kumar A, Palfrey HA, Pathak R, Kadowitz PJ, Gettys TW, Murthy SN. The metabolism and significance of homocysteine in nutrition and health. Nutr Metab (Lond). 2017;14:78. Published 2017 Dec 22. doi:10.1186/s12986-017-0233-z [PubMed]
Wu G. Amino acids: metabolism, functions, and nutrition. Amino Acids. 2009;37(1):1-17. doi:10.1007/s00726-009-0269-0 [Pubmed] [Springer]
T J de Koning. Amino acid synthesis deficiencies. J Inherit Metab Dis. 2017;40(4):609-620. doi: 10.1007/s10545-017-0063-1. [Pubmed] [Wiley] [Pubmed]
National Research Council (US) Subcommittee on the Tenth Edition of the Recommended Dietary Allowances. Recommended Dietary Allowances: 10th Edition. Washington (DC): National Academies Press (US); 1989. 6, Protein and Amino Acids. [PubMed]
Melkonian EA, Asuka E, Schury MP. Physiology, Gluconeogenesis. In: StatPearls. Treasure Island (FL): StatPearls Publishing; November 13, 2023. [Pubmed] [StatPearls]
Krajcovicová-Kudlácková, M., Blazícek, P., Kopcová, J., Béderová, A., & Babinská, K. (2000). Homocysteine levels in vegetarians versus omnivores. Annals of nutrition & metabolism, 44(3), 135–138. https://doi.org/10.1159/000012827 [PubMed] [Karger]
Ravasi G, Pelucchi S, Greni F, et al. Circulating factors are involved in hypoxia-induced hepcidin suppression. Blood Cells Mol Dis. 2014;53(4):204-210. PMID: 25065484. doi: 10.1016/j.bcmd.2014.06.006. [PubMed] [Elsevier]
Azzini E, Ruggeri S, Polito A. Homocysteine: Its Possible Emerging Role in At-Risk Population Groups. International Journal of Molecular Sciences. 2020; 21(4):1421. https://doi.org/10.3390/ijms21041421 [MDPI]
Marí M, Morales A, Colell A, García-Ruiz C, Fernández-Checa JC. Mitochondrial glutathione, a key survival antioxidant. Antioxid Redox Signal. 2009;11(11):2685-2700. doi:10.1089/ARS.2009.2695 [PubMed] [PMC Full Text] [Full Text]
Grant CM. Role of the glutathione/glutaredoxin and thioredoxin systems in yeast growth and response to stress conditions. Molecular Microbiology. 2001;39;(3):533-541. PMID 11169096. doi:10.1046/j.1365-2958.2001.02283.x. [PubMed] [Wiley]
Ha SB, Smith AP, Howden R, Dietrich WM, Bugg S, O’Connell MJ, Goldsbrough PB, Cobbett CS. Phytochelatin synthase genes from Arabidopsis and the yeast Schizosaccharomyces pombe. The Plant Cell. 1999;11(6):1153-1164. PMID 10368185. doi:10.1105/tpc.11.6.1153. [PubMed]
Dringen R. Metabolism and functions of glutathione in brain. Progress in Neurobiology. 2000;62(6):649-671. PMID 10880854. doi:10.1016/s0301-0082(99)00060-x. [PubMed] [Elsevier]
Scholz RW, Graham KS, Gumpricht E, Reddy CC. Mechanism of interaction of vitamin E and glutathione in the protection against membrane lipid peroxidation. Annals of the New York Academy of Sciences. 1989;570 (1): 514-517.PMID 14223080. doi:10.1111/j.1749-6632.1989.tb14973.x. [Wiley]
Hughes RE.. Reduction of dehydroascorbic acid by animal tissues. Nature. 1964;203(4949):1068-1069. PMID 14223080. doi:10.1038/2031068a0. [nature]
Meister A. On the enzymology of amino acid transport. Science. 1973;180(4081):33-39. PMID: 4144403. doi: 10.1126/science.180.4081.33. [Science]
Melideo, SL; Jackson, MR; Jorns, MS (22 July 2014). “Biosynthesis of a central intermediate in hydrogen sulfide metabolism by a novel human sulfurtransferase and its yeast ortholog”. Biochemistry. 53 (28): 4739–53. doi:10.1021/bi500650h. PMC 4108183. [PubMed] [PMC Full Text] [ACS Publication]
Pompella A, Visvikis A, Paolicchi A, De Tata V, Casini AF. Pompella A, Corti A. Editorial: the changing faces of glutathione, a cellular protagonist. Front Pharmacol. 2015;6:98. PMID: 26029106. doi: 10.3389/fphar.2015.00098. [PubMed] [Elsevier]
Maher TJ, Glaeser BS, Wurtman RJ. Diurnal variations in plasma concentrations of basic and neutral amino acids and in red cell concentrations of aspartate and glutamate: effects of dietary protein intake. Am J Clin Nutr. 1984;39(5):722-9. PMID: 6538743. doi: 10.1093/ajcn/39.5.722.[PubMed]
Sies H (1999). “Glutathione and its role in cellular functions”. Free Radical Biology & Medicine. 27 (9–10): 916–921. doi:10.1016/S0891-5849(99)00177-X. [PubMed] [Elsevier]
Chen Y, Yang Y, Miller ML, Shen D, Shertzer HG, Stringer KF, Wang B, Schneider SN, Nebert DW, Dalton TP (May 2007). “Hepatocyte-specific Gclc deletion leads to rapid onset of steatosis with mitochondrial injury and liver failure”. Hepatology. 45 (5): 1118–1128. doi:10.1002/hep.21635. PMID 17464988. [Semantic Scholar].
Rosolová, H., Simon, J., Mayer, O., Jr, Racek, J., Dierzé, T., & Jacobsen, D. W. (2002). Unexpected inverse relationship between insulin resistance and serum homocysteine in healthy subjects. Physiological research, 51(1), 93–98. [PubMed] [Physiological Research]
Chiang EPI, Wang YC, Chen WW, Tang FY. Effects of Insulin and Glucose on Cellular Metabolic Fluxes in Homocysteine Transsulfuration, Remethylation,S-Adenosylmethionine Synthesis, and Global Deoxyribonucleic Acid Methylation. The Journal of Clinical Endocrinology & Metabolism. 2009;94(3):1017-1025. doi:https://doi.org/10.1210/jc.2008-2038 [Research Gate]
Cascalheira JF, Parreira MC, Viegas AN, Faria MC, Domingues FC. Serum homocysteine: relationship with circulating levels of cortisol and ascorbate. Ann Nutr Metab. 2008;53(1):67-74. doi:10.1159/000158636 [PubMed] [Karger]
Koenig G, Seneff S. Gamma-glutamyltransferase: A predictive biomarker of cellular antioxidant inadequacy and disease risk. Dis Markers. 2015:2015:818570. PMID: 26543300. doi: 10.1155/2015/818570. [PubMed] [Wiley] [PubMed]
Zaric BL, Obradovic M, Bajic V, Haidara MA, Jovanovic M, Isenovic ER. Homocysteine and Hyperhomocysteinaemia. Curr Med Chem. 2019;26(16):2948-2961. doi:10.2174/0929867325666180313105949 [PubMed] [BenthamScience]
Zhang H, Tsao R. Dietary polyphenols, oxidative stress and antioxidant and anti-inflammatory effects. Current Opinion in Food Science. 2016;8:33-42. doi:10.1016/j.cofs.2016.02.002 [Elsevier]
Hurrell R, Egli I. Iron bioavailability and dietary reference values. Am J Clin Nutr. 2010;91(5):1461S-1467S. doi: 10.3945/ajcn.2010.28674F [PubMed] [Elsevier]
Cory, H., Passarelli, S., Szeto, J., Tamez, M., & Mattei, J. (2018). The Role of Polyphenols in Human Health and Food Systems: A Mini-Review. Frontiers in nutrition, 5, 87. https://doi.org/10.3389/fnut.2018.00087 [PubMed]
Desai A, Sequeira JM, Quadros EV. The metabolic basis for developmental disorders due to defective folate transport. Biochimie. 2016;126:31-42. doi:10.1016/j.biochi.2016.02.012 [PubMed] [Elsevier]
Moll S, Varga EA. Homocysteine and MTHFR Mutations. Circulation. 2015;132(1). doi:https://doi.org/10.1161/circulationaha.114.013311 [AHA Journals]
O’Callaghan, P., Meleady, R., Fitzgerald, T., Graham, I., & European COMAC group (2002). Smoking and plasma homocysteine. European heart journal, 23)20), 1580-1586.[PubMed] [OxfordAcademic]
Slyepchenko A, Brunoni AR, McIntyre RS, Quevedo J, Carvalho AF. The Adverse Effects of Smoking on Health Outcomes in Bipolar Disorder: A Review and Synthesis of Biological Mechanisms. Current Molecular Medicine. 2016;16(2):187-205. doi:https://doi.org/10.2174/1566524016666160126144601 [Research Gate]
Kamat, P. K., Mallonee, C. J., George, A. K., Tyagi, S. C., & Tyagi, N. (2016). Homocysteine, Alcoholism, and Its Potential Epigenetic Mechanism. Alcoholism, clinical and experimental research, 40(12), 2474–2481. https://doi.org/10.1111/acer.13234 [PubMed
Desouza C, Keebler M, McNamara DB, Fonseca V. Drugs Affecting Homocysteine Metabolism. Drugs. 2002;62(4):605-616. doi:https://doi.org/10.2165/00003495-200262040-00005 [Springer]
Larrey D, Pageaux GP. Drug-induced acute liver failure. Eur J Gastroenterol Hepatol. 2005;17(2):141-143. doi:10.1097/00042737-200502000-00002 [PubMed] [Crosslink]
Fontana RJ, Hayashi PH, Gu J, et al. Idiosyncratic drug-induced liver injury is associated with substantial morbidity and mortality within 6 months from onset. Gastroenterology. 2014;147(1):96-108.e4. doi:10.1053/j.gastro.2014.03.045 [PMC Full Text] [PubMed] [Crosslink]
McGill MR, Jaeschke H. Metabolism and disposition of acetaminophen: recent advances in relation to hepatotoxicity and diagnosis. Pharm Res. 2013;30(9):2174-2187. doi:10.1007/s11095-013-1007-6 [PMC Full Text] [PubMed] [Crosslink]
McGill MR, Sharpe MR, Williams CD, Taha M, Curry SC, Jaeschke H. The mechanism underlying acetaminophen-induced hepatotoxicity in humans and mice involves mitochondrial damage and nuclear DNA fragmentation. J Clin Invest. 2012;122(4):1574-1583. doi:10.1172/JCI59755 [PMC Full Text] [PubMed] [Crosslink]
Watkins PB, Kaplowitz N, Slattery JT, et al. Aminotransferase elevations in healthy adults receiving 4 grams of acetaminophen daily: a randomized controlled trial. JAMA. 2006;296(1):87-93. doi:10.1001/jama.296.1.87 [PubMed] [Crosslink]
Yuan L, Kaplowitz N. Mechanisms of drug-induced liver injury. Clin Liver Dis. 2013;17(4):507-vii. doi:10.1016/j.cld.2013.07.002 [PMC Full Text] [PubMed] [Crosslink]
Harshad Devarbhavi, Raj S, Aradya VH, et al. Drug‐induced liver injury associated with stevens‐Johnson syndrome/toxic epidermal necrolysis: Patient characteristics, causes, and outcome in 36 cases. 2016;63(3):993-999. doi:https://doi.org/10.1002/hep.28270 [AASLD]
Kaplowitz N. Idiosyncratic drug hepatotoxicity. Nat Rev Drug Discov. 2005;4(6):489-499. doi:10.1038/nrd1750 [PubMed] [Crosslink]
Russmann S, Jetter A, Kullak-Ublick GA. Pharmacogenetics of drug-induced liver injury. Hepatology. 2010;52(2):748-761. doi:10.1002/hep.23720 [PubMed] [Crosslink] [Google Scholar]
Lalouschek, W., Aull, S., Serles, W., Schnider, P., Mannhalter, C., Lang, T., Deecke, L., & Zeiler, K. (1999). Genetic and nongenetic factors influencing plasma homocysteine levels in patients with ischemic cerebrovascular disease and in healthy control subjects. The Journal of laboratory and clinical medicine, 133(6), 575–582. https://doi.org/10.1016/s0022-2143(99)90187-7 [PubMed] [Elsevier]
Kraus, J. P., Janosík, M., Kozich, V., Mandell, R., Shih, V., Sperandeo, M. P., Sebastio, G., de Franchis, R., Andria, G., Kluijtmans, L. A., Blom, H., Boers, G. H., Gordon, R. B., Kamoun, P., Tsai, M. Y., Kruger, W. D., Koch, H. G., Ohura, T., & Gaustadnes, M. (1999). Cystathionine beta-synthase mutations in homocystinuria. Human mutation, 13(5), 362–375.[PubMed] [Wiley]
Scalise V, Balia C, Cianchetti S, et al. Non enzymatic upregulation of tissue factor expression by gamma-glutamyl transferase in human peripheral blood mononuclear cells. Thromb J. 2016;14:45. Published 2016 Nov 4. doi:10.1186/s12959-016-0119-8 [PubMed]
Guoyao Wu; Yun-Zhong Fang; Sheng Yang; Joanne R. Lupton; Nancy D. Turner (2004). “Glutathione Metabolism and its Implications for Health”. Journal of Nutrition. 134 (3): 489–492. doi:10.1093/jn/134.3.489. PMID 14988435
Song Y, Liu J, Zhao K, Gao L, Zhao J. Cholesterol-induced toxicity: An integrated view of the role of cholesterol in multiple diseases. Cell Metabolism. 2021;33(10):1911-1925. doi:10.1016/j.cmet.2021.09.001 [Elsevier]
Chen P, Poddar R, Tipa EV, et al. Homocysteine metabolism in cardiovascular cells and tissues: implications for hyperhomocysteinemia and cardiovascular disease. Adv Enzyme Regul. 1999:39:93-109. PMID: 10470368 DOI: 10.1016/s0065-2571(98)00029-6. [PubMed]
Abhijit Basu A, Dvorina N, Baldwin W, Mazumder B. High‐fat diet‐induced GAIT element‐mediated translational silencing of mRNAs encoding inflammatory proteins in macrophage protects against atherosclerosis. FASEB Journal. March 2020; 34(5). DOI:10.1096/fj.201903119R
Tiedge M., Lortz S., Drinkgern J., Lenzen S. Relation between antioxidant enzyme gene expression and antioxidative defense status of insulin-producing cells. Diabetes. 1997;46:1733–1742. doi: 10.2337/diab.46.11.1733. [PubMed] [CrossRef] [Google Scholar]
Esse R, Barroso M, Tavares de Almeida I, Castro R. The Contribution of Homocysteine Metabolism Disruption to Endothelial Dysfunction: State-of-the-Art. Int J Mol Sci. 2019;20(4):867. Published 2019 Feb 17. doi:10.3390/ijms20040867 [PubMed] [MDPI] [PubMed]
Viroonudompho D, Kanjanachumpol S, Sirisate S. Homocysteine, vitamin B12 and folic acid in children with acute glomerulonephritis. World J Eng Technol. 2018;6:661-670. DOI:10.4236/wjet.2018.63042. [Scientific Research]
Perna AF, Ingrosso D. Atherosclerosis determinants in renal disease: How much is homocysteine involved? Nephrol Dial Transplant. 2016;31(6):860-863. PMID: 26687901. doi: 10.1093/ndt/gfv409. [PubMed] [OxfordAcademic]
Behera J, Bala J, Nuru M, Tyagi SC, Tyagi N. Homocysteine as a Pathological Biomarker for Bone Disease. J Cell Physiol. 2017;232(10):2704-2709. doi:10.1002/jcp.25693 [PubMed]
Narvaez J, Maldonado G, Intriago M, et al. Role of homocysteine and vitamin B in bone metabolism. 2020;27(4):278-285. doi:https://doi.org/10.1016/j.rcreue.2019.12.008 [Elsevier]
Ajith TA, Ranimenon. Homocysteine in ocular diseases. Clin Chim Acta. 2015;450:316-321. doi:10.1016/j.cca.2015.09.007 [PubMed] [Elsevier]
Irizarry MC, Gurol ME, Raju S, et al. Association of homocysteine with plasma amyloid beta protein in aging and neurodegenerative disease. Neurology. 2005;65(9):1402-8. PMID: 16275827. doi: 10.1212/01.wnl.0000183063.99107.5c. [PubMed] [Neurology]
Ho PI, Ashline D, Dhitavat S, et al. Folate deprivation induces neurodegeneration: roles of oxidative stress and increased homocysteine. Neurobiol Dis. PMID: 13678664. 2003;14(1):32-42. doi: 10.1016/s0969-9961(03)00070-6. [Elsevier]
Kruman II, Culmsee C, Chan SL, et al. Homocysteine elicits a DNA damage response in neurons that promotes apoptosis and hypersensitivity to excitotoxicity. J Neurosci. 2000;20:6920-6926. PMID: 10995836 PMCID: DOI: 10.1523/JNEUROSCI.20-18-06920.2000. [PubMed] [JNeurosci] [PubMed]
Fuentes-Albero M, Cauli O. Homocysteine Levels in Autism Spectrum Disorder: A Clinical Update. Endocr Metab Immune Disord Drug Targets. 2018;18:289-296. PMID: 29437021 DOI: 10.2174/1871530318666180213110815. [PubMed] [BenthamScience]
Mattson MP, Shea TB. Folate and homocysteine metabolism in neural plasticity and neurodegenerative disorders. Trends Neurosci. 2003;26:137-146. PMID: 12591216. DOI: 10.1016/S0166-2236(03)00032-8.. [PubMed] [CellPress]
Rossignol DA, Frye RE. Evidence linking oxidative stress, mitochondrial dysfunction, and inflammation in the brain of individuals with autism. Front Physiol. 2014:5:150. PMID: 24795645. doi: 10.3389/fphys.2014.00150. [PubMed] [Frontiers] [PubMed]
Setién-Suero E, Suárez-Pinilla M, Suárez-Pinilla P, Crespo-Facorro B, Ayesa-Arriola R. Homocysteine and cognition: A systematic review of 111 studies. Neurosci Biobehav.Rev. 2016:69:280-98. PMID: 27531233. doi:10.1016/j.neubiorev.2016.08.014. [PubMed] [Elsevier]
Kanjwal Y, Kosinski D, Grubb BP. The postural orthostatic tachycardia syndrome: definitions, diagnosis, and management. Pacing Clin Electrophysiol. 2003;26(8):1747-1757. PMID: 12877710. DOI: 10.1046/j.1460-9592.2003.t01-1-00262.x. [PubMed] [Wiley]
Li Y, He B, Li H, Zhang Q, Tang C, Du J, Jin H. Plasma homocysteine level in children with postural tachycardia syndrome. Front Pediatr. 2018;6:375. PMID: 3056010. DOI: 10.3389/fped.2018.00375.. [PubMed]
Shen WK, Sheldon RS, Benditt DG, et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2017;70:e39-e110. PMID: 28286221. DOI: 10.1016/j.jacc.2017.03.003. [PubMed] [AHAJournal]
El-Amrousy D, Hassan S, Hodeib H. Prognostic value of homocysteine and highly sensitive cardiac troponin T in children with acute heart failure. J Saudi Heart Assoc. 2018;30(3):198-204. doi:10.1016/j.jsha.2017.11.007 [PubMed]
Schaffer A, Verdoia M, Cassetti E, et al. Relationship between homocysteine and coronary artery disease. Results from a large prospective cohort study. Thromb Res. 2014;134(2):288-293. doi:10.1016/j.thromres.2014.05.025 [PubMed] [Elsevier]
Ganguly P, Alam SF. Role of homocysteine in the development of cardiovascular disease. Nutr J. 2015;14:6. Published 2015 Jan 10. doi:10.1186/1475-2891-14-6 [PubMed]
Lehotský J, Tothová B, Kovalská M, et al. Role of Homocysteine in the Ischemic Stroke and Development of Ischemic Tolerance. Front Neurosci. 2016;10:538. Published 2016 Nov 23. doi:10.3389/fnins.2016.00538 [PubMed]
Bergen N, Jaddoe V, Timmermans S, et al. Homocysteine and folate concentrations in early pregnancy and the risk of adverse pregnancy outcomes: The Generation R Study. BJOG. 2012;119:739-751. PMID: 30053452. DOI: 10.1016/j.cbi.2018.07.021.. [PubMed] [Wiley]
Peker E, Demir N, Tuncer O, et al. The levels of vitamın B12, folate and homocysteine in mothers and their babies with neural tube defects. The Journal of Maternal-Fetal & Neonatal Medicine. Published online November 23, 2015:1-5. doi:https://doi.org/10.3109/14767058.2015.1109620 [Tandfonline]
Yang M, Li W, Wan Z, Du Y. Elevated homocysteine levels in mothers with neural tube defects: a systematic review and meta-analysis. J Matern Fetal Neonatal Med. 2017;30:2051-2057. PMID: 27633659. DOI: 10.1080/14767058.2016.1236248.. [PubMed] [Tandfonline]
Murphy MM, Fernadez-Ballart, JD. Homocysteine in pregnancy. Adv Clin Chem. 2011;53:105-107. PMID: 21404916. DOI: 10.1016/b978-0-12-385855-9.00005-9.. [PubMed]
Gaiday AN, Tussupkaliyev ABT, Bermagambetova SK, et al.Effect of homocysteine on pregnancy: A systematic review. Chem Biol Interact. 2018;293:70-76. PMID: 30053452. DOI: 10.1016/j.cbi.2018.07.021. [PubMed] [Elsevier]
Gupta R, Kumari P, Pandey S, et al. Homocysteine and vitamin B12: Other causes of neural tube defects in Eastern Uttar Pradesh and Western Bihar population. Neurol India. 2018;66:1016-1019. PMID: 30038085. DOI: 10.4103/0028-3886.236968.. [PubMed] [Wolters]
Kennedy RH, Owings R, Shekhawat, N, Joseph, J. Acute negative inotropic effects of homocysteine are mediated via the endothelium. Am J Physiol Heart Circ Physiol. 2004;287(2):H812-7. doi: 10.1152/ajpheart.01042.2003.. [American Journal of Physiology]
Laskowska M, Oleszczuk J. Homocysteine in pregnancies complicated by preeclampsia with and without IUGR: A comparison with normotensive pregnant women with isolated IUGR and healthy pregnant women. Open J Obstet Gynecol. 2011;1:191-196. PMID: 27633659. DOI: 10.1080/14767058.2016.1236248. [Research Gate]
Selhub, J., Jacques, P. F., Wilson, P. W., Rush, D., & Rosenberg, I. H. (1993). Vitamin status and intake as primary determinants of homocysteinemia in an elderly population. JAMA, 270(22), 2693–2698. https://doi.org/10.1001/jama.1993.03510220049033 [PubMed] [JAMA]
Walker MC, Smith GN, Perkins SL, Keely EJ, Garner PR. Changes in homocysteine levels during normal pregnancy. American Journal of Obstetrics and Gynecology. 1999;180(3):660-664. doi:https://doi.org/10.1016/s0002-9378(99)70269-3 [Elsevier] [AJOG]
Pogribna, M., Melnyk, S., Pogribny, I., Chango, A., Yi, P., & James, S. J. (2001). Homocysteine metabolism in children with Down syndrome: in vitro modulation. American journal of human genetics, 69(1), 88–95. https://doi.org/10.1086/321262 [PubMed]
Kumar N, Gane B, Rao R, Bhat V. Folate and Homocysteine metabolism in Indian children with Down syndrome. Curr Pediatr Res. 2014;18(1):11-14. Accessed August 1, 2024. [ABAAcademies]
Bergen N, Jaddoe V, Timmermans S, et al. Homocysteine and folate concentrations in early pregnancy and the risk of adverse pregnancy outcomes: The Generation R Study. BJOG. 2012;119:739-751. PMID: 30053452. DOI: 10.1016/j.cbi.2018.07.021.. [PubMed] [Wiley]
Yang Y, Zeng Y, Yuan S, et al. Prevalence and risk factors for hyperhomocysteinemia: a population-based cross-sectional study from Hunan, China. BMJ Open. 2021;11(12):e048575. Published 2021 Dec 6. doi:10.1136/bmjopen-2020-048575 [PubMed]
Fan, R., Zhang, A., & Zhong, F. (2017). Association between Homocysteine Levels and All-cause Mortality: A Dose-Response Meta-Analysis of Prospective Studies. Scientific reports, 7(1), 4769. https://doi.org/10.1038/s41598-017-05205-3 [PubMed]
Brustolin, S., Giugliani, R., & Félix, T. M. (2010). Genetics of homocysteine metabolism and associated disorders. Brazilian journal of medical and biological research = Revista brasileira de pesquisas medicas e biologicas, 43(1), 1–7. https://doi.org/10.1590/s0100-879×2009007500021 [PubMed]
Challa, F., Getahun, T., Sileshi, M., Nigassie, B., Geto, Z., Ashibire, G., Gelibo, T., Teferra, S., Seifu, D., Sitotaw, Y., Bekele, A., Abate, E., & Baye, K. (2020). Prevalence of Hyperhomocysteinaemia and Associated Factors among Ethiopian Adult Population in a 2015 National Survey. BioMed research international, 2020, 9210261. https://doi.org/10.1155/2020/9210261 [PubMed]
Kamdi, S. P., & Palkar, P. (2013). Prevalence of hyperhomocysteinemia in healthy Indian doctors. Bioinformation, 9(4), 193–196. https://doi.org/10.6026/97320630009193 [PubMed] [PubMed]
Krishnaswamy, K., & Lakshmi, A. V. (2002). Role of nutritional supplementation in reducing the levels of homocysteine. The Journal of the Association of Physicians of India, 50 Suppl, 36–42. [PubMed]
Ramsay DJ. Homeostatic control of water balance. In: Arnaud MJ, editor. Hydration Throughout Life. Montrouge: John Libbey Eurotext; 1998. pp. 9–18. [Google Scholar]
Maroto-Sánchez, B., Lopez-Torres, O., Valtueña, J., Benito, P. J., Palacios, G., Díaz-Martínez, Á. E., González-Lamuño, D., Zinellu, A., González-Gross, M., & Carru, C. (2019). Rehydration during exercise prevents the increase of homocysteine concentrations. Amino acids, 51(2), 193–204. https://doi.org/10.1007/s00726-018-2655-y [PubMed] [Springer]
Deminice R, Ribeiro DF, Frajacomo FT. The Effects of Acute Exercise and Exercise Training on Plasma Homocysteine: A Meta-Analysis. PLoS One. 2016;11(3):e0151653. Published 2016 Mar 17. doi:10.1371/journal.pone.0151653 [PubMed]
Steenge GR, Verhoef P, Katan MB. Betaine supplementation lowers plasma homocysteine in healthy men and women. J Nutr. 2003;133(5):1291-1295. PMID: 12730412. doi: 10.1093/jn/133.5.1291. [PubMed]
Olthof, M. R., van Vliet, T., Boelsma, E., & Verhoef, P. (2003). Low dose betaine supplementation leads to immediate and long term lowering of plasma homocysteine in healthy men and women. The Journal of nutrition, 133(12), 4135–4138. https://doi.org/10.1093/jn/133.12.4135 [PubMed]
National Institutes of Health. Office of Dietary Supplements – Folate. Nih.gov. Published November 30, 2022. https://ods.od.nih.gov/factsheets/Folate-HealthProfessional/ [National Institutes of Health]
Hanna M, Jaqua E, Nguyen V, Clay J. B Vitamins: Functions and Uses in Medicine. Perm J. 2022;26(2):89-97. doi:10.7812/TPP/21.204 [PubMed] [PMC Full Text] [Crosslink]
Jones L. Vitamin B12 for Vegans & Vegetarians: Best Natural Sources. Fresh N Lean. June 1, 2023. Accessed July 4, 2024.
McRae MP. Betaine supplementation decreases plasma homocysteine in healthy adult participants: a meta-analysis. J Chiropr Med. 2013;12(1):20-25. PMID: 23997720. doi: 10.1016/j.jcm.2012.11.001. [PubMed] [Elsevier] [PubMed]
Witschi A, Reddy S, Stofer B, Lauterburg BH. The systemic availability of oral glutathione. Eur J Clin Pharmacol. 1992;43(6):667-669. doi: 10.1007/BF02284971. [PubMed] [Springer]
ASHP, Acetylcysteine (Monograph). https://www.drugs.com/monograph/acetylcysteine.html. Medically reviewed by Drugs.com on Aug 22, 2023. [Drugs.com]
Nagasawa, Herbert T. (27 November 2014). “Compositions comprising sugar-cysteine products – US-20140348811-A1”. ppubs.uspto.gov. United States Patent Office. p. 16. Retrieved 31 October 2023. 30. A method of increasing ATP and/or glutathione.” [PPUBS]
Ukwenya VO, Alese MO, Ogunlade B, Folorunso IM, Omotuyi OI (2022). “Anacardium occidentale leaves extract and riboceine mitigate hyperglycemia through anti-oxidative effects and modulation of some selected genes associated with diabetes”. J Diabetes Metab Disord. 22 (1): 455–468. [PubMed] [Springer] [Full Text]
Betaine Information | Mount Sinai – New York. Mount Sinai Health System. Accessed July 29, 2024. [Mount Sinai]
Betaine (Oral Route) Proper Use – Mayo Clinic. www.mayoclinic.org. Accessed July 29, 2024. [Mayo Clinic]
Ghasemian M, Owlia S, Owlia MB. Review of Anti-Inflammatory Herbal Medicines. Adv Pharmacol Sci. 2016;2016:9130979. doi:10.1155/2016/9130979 [PubMed]