
Platelets: Diagnostic Significance and Clinical Insights
Authors: Payal Bhandari M.D, Emilia Feria, Madison Granados
Contributors: Vivi Chador, Amer Džanković
Key Insights
Platelets are small cell fragments that play a key role in stopping bleeding and healing wounds. They release proteins that support the immune system, repair tissue, and keep blood vessels healthy. Platelets are continuously produced and released into the bloodstream, with their function tightly regulated by thrombopoietin and influenced by oxygen levels, inflammation, and blood flow. Problems with platelet production or function can lead to serious health issues. Low platelet counts (thrombocytopenia) increase bleeding risk, while high counts (thrombocytosis) may cause blood clots. These conditions are often linked to low oxygen levels, rapid red blood cell breakdown, or inflammation, which can contribute to vascular diseases, infections, or even cancer spread. Tests like the platelet count and mean platelet volume (MPV) provide insights into platelet quantity and size, helping assess their activity. A thorough medical history, lab tests, and genetic testing can identify inherited or acquired platelet disorders, enabling personalized treatments that improve health outcomes.1
What Are Platelets?
Platelets, also called thrombocytes, are the smallest cell fragments in the blood and lack a nucleus. When inactive, they resemble tiny plates visible only under a microscope. Measuring just 2 to 3 micrometers in diameter, they are similar in size to white blood cells but are only about 20% the size of red blood cells.
Role of Platelets
Blood comprises three types of cells: red blood cells (RBCs), white blood cells (WBCs), and platelets. They all originate from the bone marrow and have critical functions:
RBCs contain hemoglobin, giving blood its red color and transporting oxygen to tissues.
WBCs are the body’s immune defense.
Platelets stop bleeding by forming a plug, repairing injury sites, preventing blood loss, and creating new blood vessels.
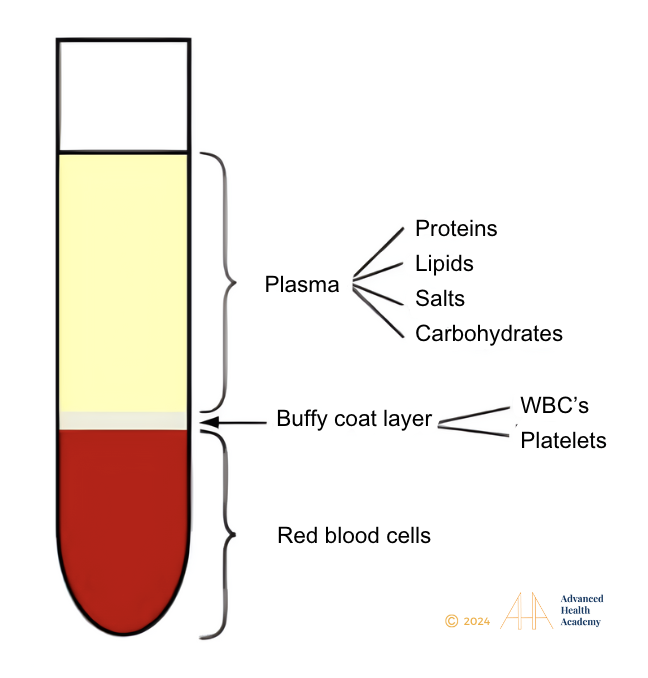
Figure 1: Blood is divided into three parts: 55% is plasma, which comprises water (93%), salts, proteins, lipids, and glucose; 45% are RBCs; and 1% are WBCs and platelets.
Factors that initiate a blood clot are:
Damaged blood vessels
Inflammation of blood vessels
Impaired blood flow
Primary Clot Formation:
Adhesion: When a blood vessel is injured, subendothelial collagen and von Willebrand vWH factor (vWF) are exposed, stimulating platelets to rush to the injury site.
Activation: When platelets contact a damaged blood vessel, they bind to GP Ib-IX-V and vWF receptors. This triggers them to form sticky, tentacle-like extensions, helping create a clot (thrombus) over the injury.
Secretion: Platelet Activation: Activation triggers signaling cascades (PLC, PKC, calcium), causing platelets to change shape, release granule contents (vWF, fibrinogen, ADP, calcium), and recruit more platelets to strengthen the clot.
Aggregation: Fibrinogen binds to GP IIb/IIIa receptors on platelets, enabling them to connect and form a platelet plug.
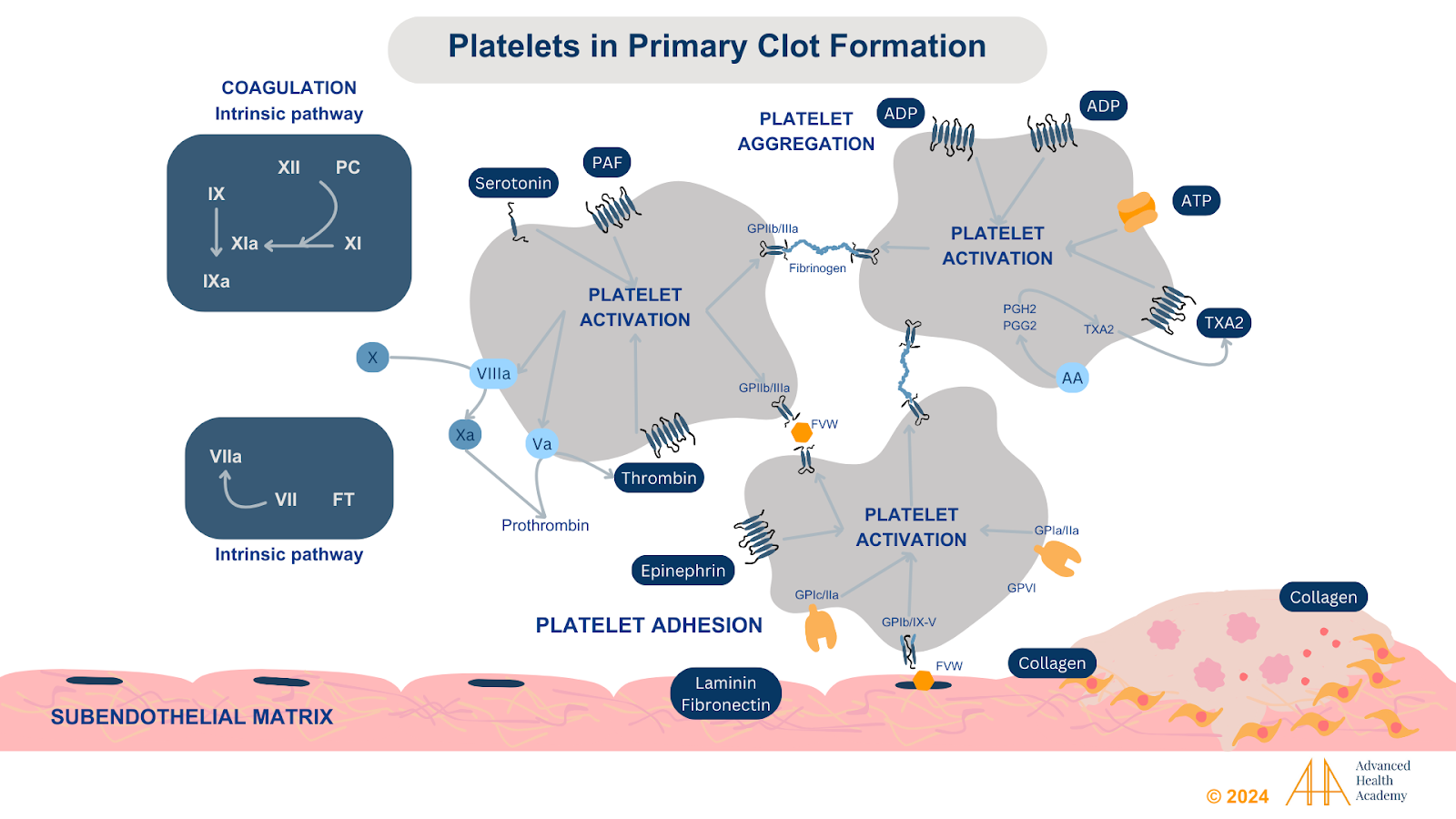
Figure 2: Diagram of platelet activation, adhesion, coagulation, and further aggregation.
Secondary Clot Formation and Stabilization
After forming the initial platelet plug, activated platelets release four procoagulants (PF1–PF4) to strengthen the clot and seal vessel breaks. Thrombin converts fibrinogen into fibrin, a protein that weaves into the plug to create a stable clot, like a scab.8 Platelets also provide a phospholipid surface for coagulation factors to assemble and form a thrombus.
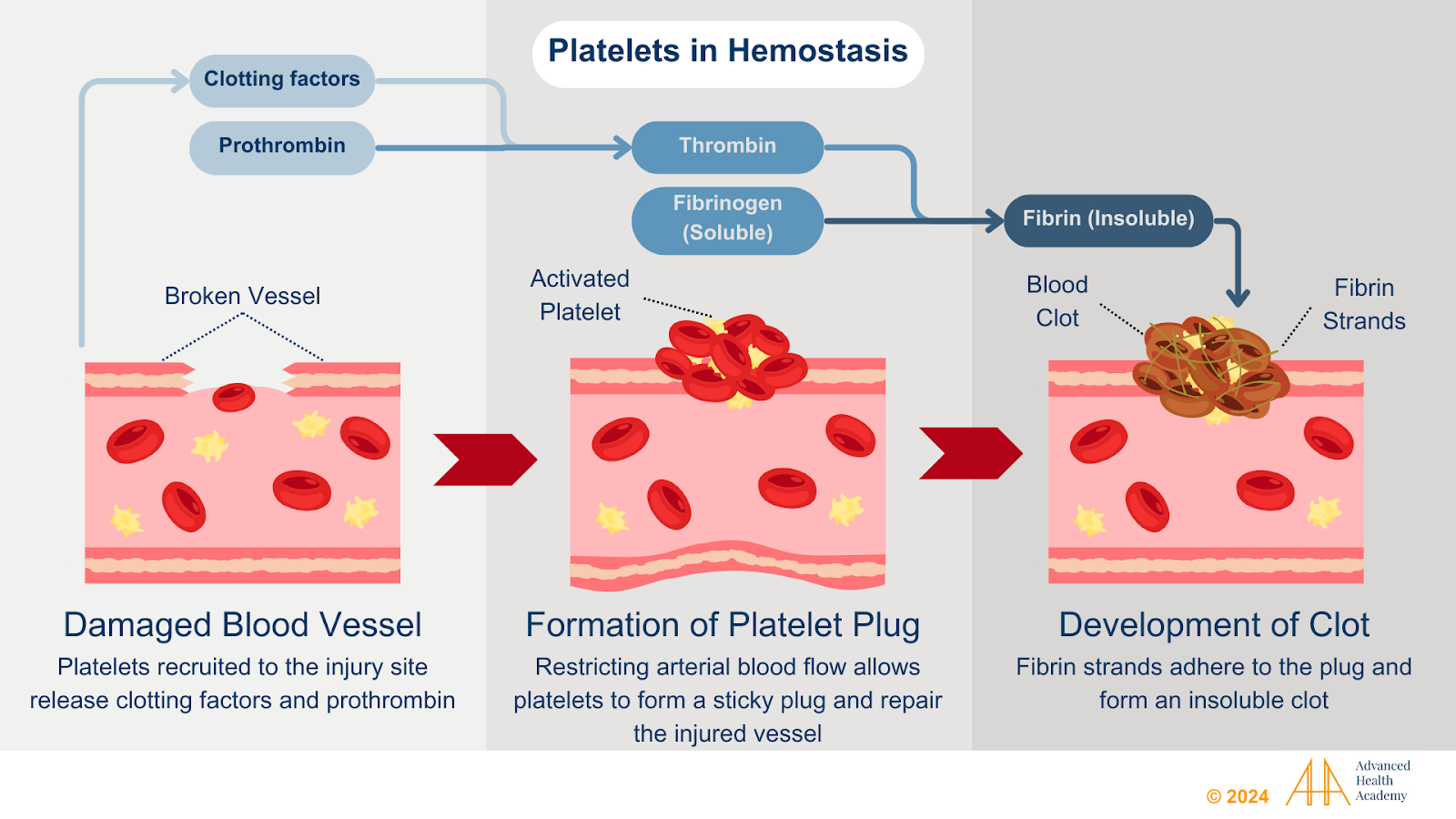
Figure 3: Distinct phases of platelet function in primary hemostasis and thrombosis. Platelets adhere to vascular damage, change shape, secrete granules, and recruit more platelets for aggregation. Insoluble fibrin forms and cross-links to stabilize the platelet plug.
Additional Roles of Platelets
Wound healing: Platelets release growth factors like PDGF and TGF-beta, which aid in repairing blood vessels, stimulating cell division, supporting tissue growth, and remodeling. These processes include forming bone, tendons, and new blood vessels (angiogenesis).
Inflammation: Platelets release chemokines and cytokines, recruiting white blood cells and endothelial cells to injury or infection sites.
Tumor growth and metastasis:34 Platelets help cancer cells bind to the endothelium and support their growth and metastasis.
Immune Defense9: Platelets are key players in the immune system, constantly fighting pathogens, cancer cells, and invaders. They release antimicrobial peptides that attract neutrophils and monocytes to inflammation sites. These white blood cells adhere to and destroy microbes, clear debris, and produce antibodies to combat invaders.
Origin and Formation of Platelets
Red blood cells (RBCs), white blood cells (WBCs), and platelets come from hematopoietic stem cells in the bone marrow, found in flat bones like the skull, ribs, pelvis, and sternum. Lymphatic tissues in the thymus, spleen, liver, and lymph nodes provide oxygen and nutrients to help stem cells develop into specific cell types:
Proerythroblasts: Produce RBCs.
Hemocytoblasts: Produce WBCs.
Megakaryoblasts: Produce megakaryocytes and platelets.
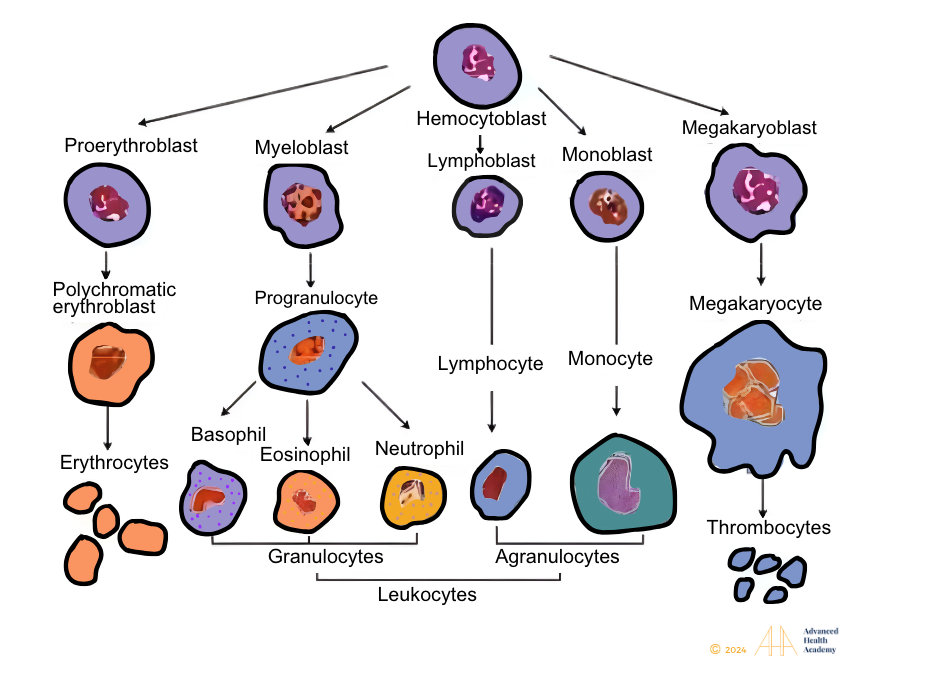
Figure 4: Red blood cells, white blood cells, and platelets originate from stem cells in the bone marrow.
MKs release thousands of platelets into the bloodstream. Platelets then circulate for 8 to 10 days before being cleared by the spleen and liver.
Regulation of Platelet Formation
Low oxygen levels (hypoxia) speed up red blood cell (RBC) destruction (hemolysis), prompting the kidneys to release erythropoietin (EPO), which regulates RBC production. Prolonged hypoxia reduces EPO and slows RBC production. Platelet production, however, remains unaffected by hypoxia. The liver and kidneys produce thrombopoietin (TPO) and CFU-meg, which convert myeloid stem cells into megakaryoblasts, megakaryocytes, and platelets in the bone marrow. MKs are large cells that stay in the bone marrow. Blood flow shears off foot-like projections from their cytoplasm, forming platelets.
Rarely, whole megakaryocytes (MKs) leave the bone marrow and enter the bloodstream, traveling to the lungs. In the lung capillaries, low oxygen levels can prevent their conversion into platelets. Chronic inflammation with high reactive oxygen species (ROS) boosts MK conversion to platelets in lung tissue, promoting thrombus formation. TPO and CFU-meg binding to circulating MKs increase MK destruction and reduce platelet production in the bone marrow.
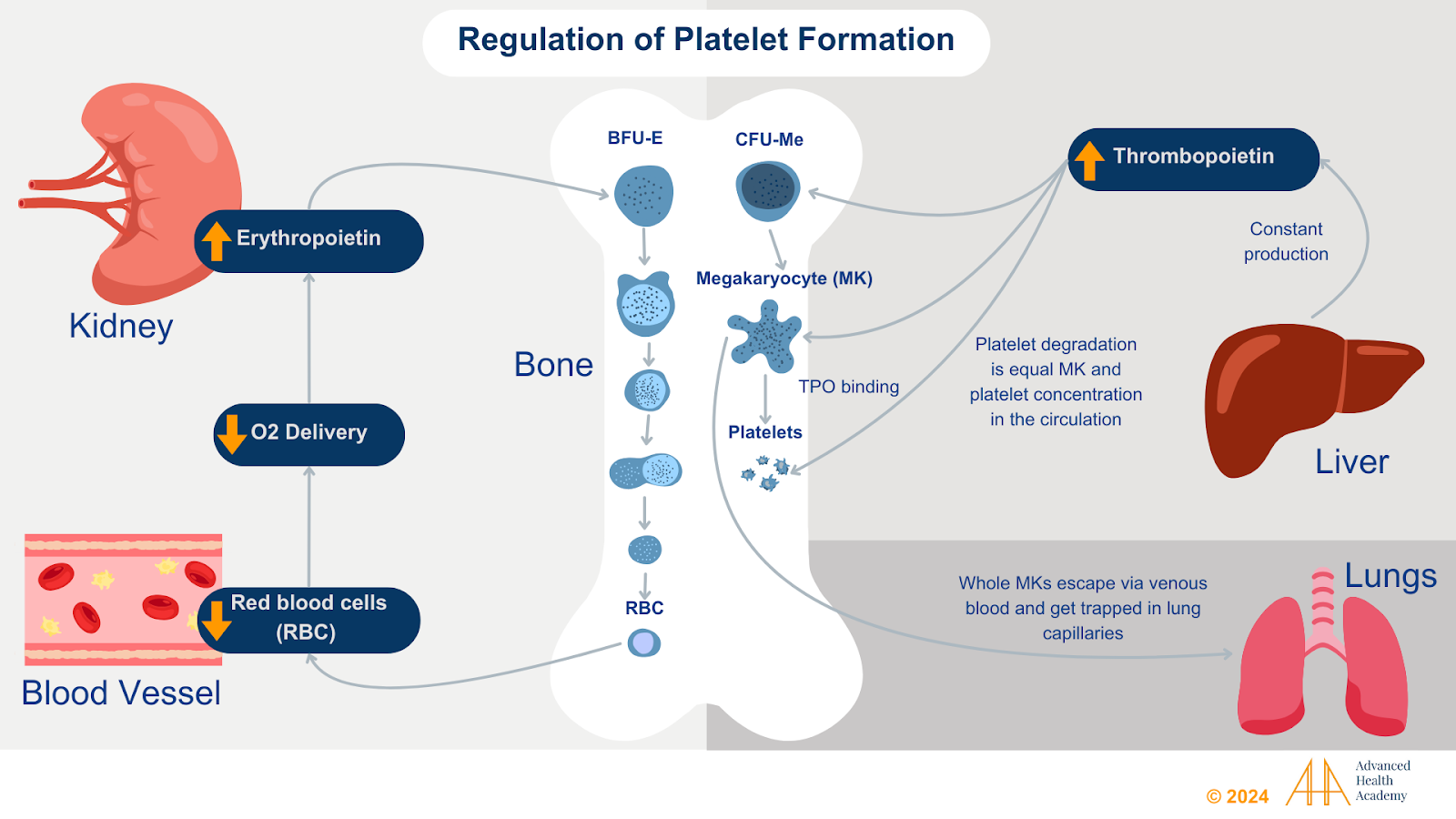
Figure 5: Decreased blood oxygen increases red blood cell production and whole megakaryocytes (MK) escape the bone marrow and travel to the lungs. Increased blood oxygen converts lung MKs to platelets, which are quickly destroyed. Chronic inflammation accelerates platelet breakdown, reducing liver thrombopoietin and bone marrow platelet production.
Clinical Significance of Monitoring Platelet Levels
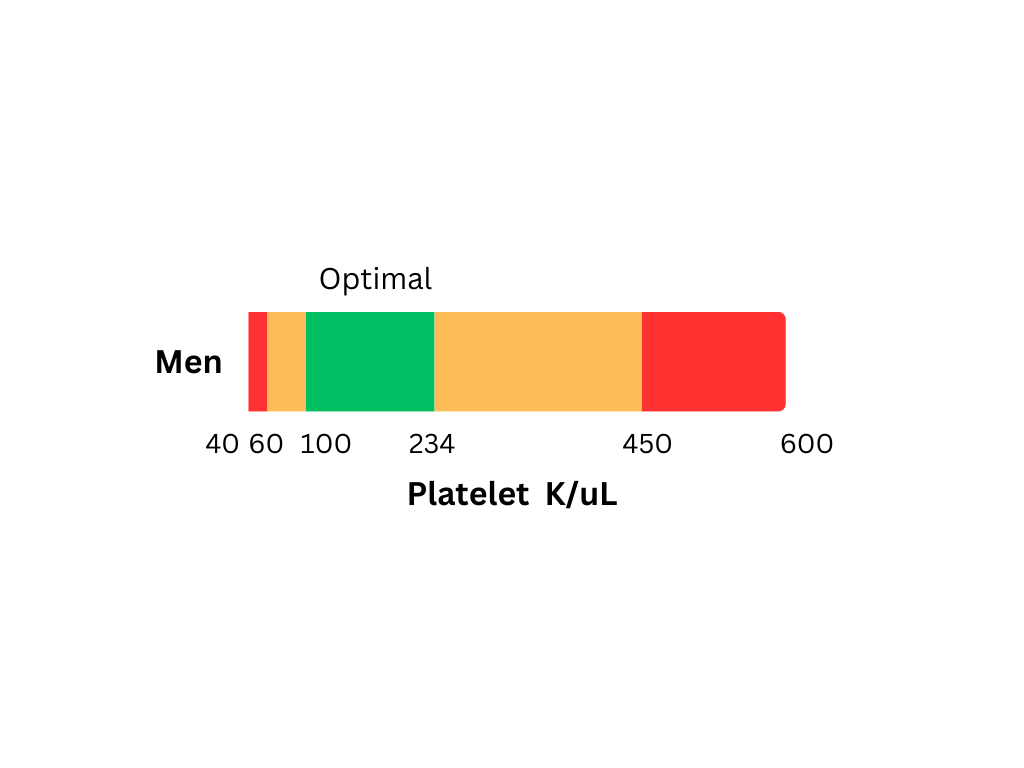
The platelet count test measures the total number of “inactive” platelets (thrombocytes) in the blood.
Thrombocytopenia (Low Platelet Count)
Thrombocytopenia, a low platelet count, results from increased clotting and MK destruction, reducing platelets and raising bleeding risk.
The leading cause of thrombocytopenia is excess fluid loss (dehydration) and its direct impact on the gut microbiota. TGut bacteria aid in digestion, nutrient absorption, protein synthesis (like hemoglobin), energy harvesting, hormone production, and waste removal.,, Dehydration reduces plasma volume, raising ion concentrations outside cells. This causes water loss in red blood cells (RBCs), shrinking them and reducing oxygen delivery (hypoxia). Chronic dehydration damages RBCs and speeds up their clearance. Conversely, excess ions inside cells pull in water, causing RBCs to swell and burst. Both scenarios accelerate hemolysis, overwhelming the body’s ability to clear damaged RBCs and increasing reactive oxygen species (ROS) and proinflammatory proteins like cytokines.
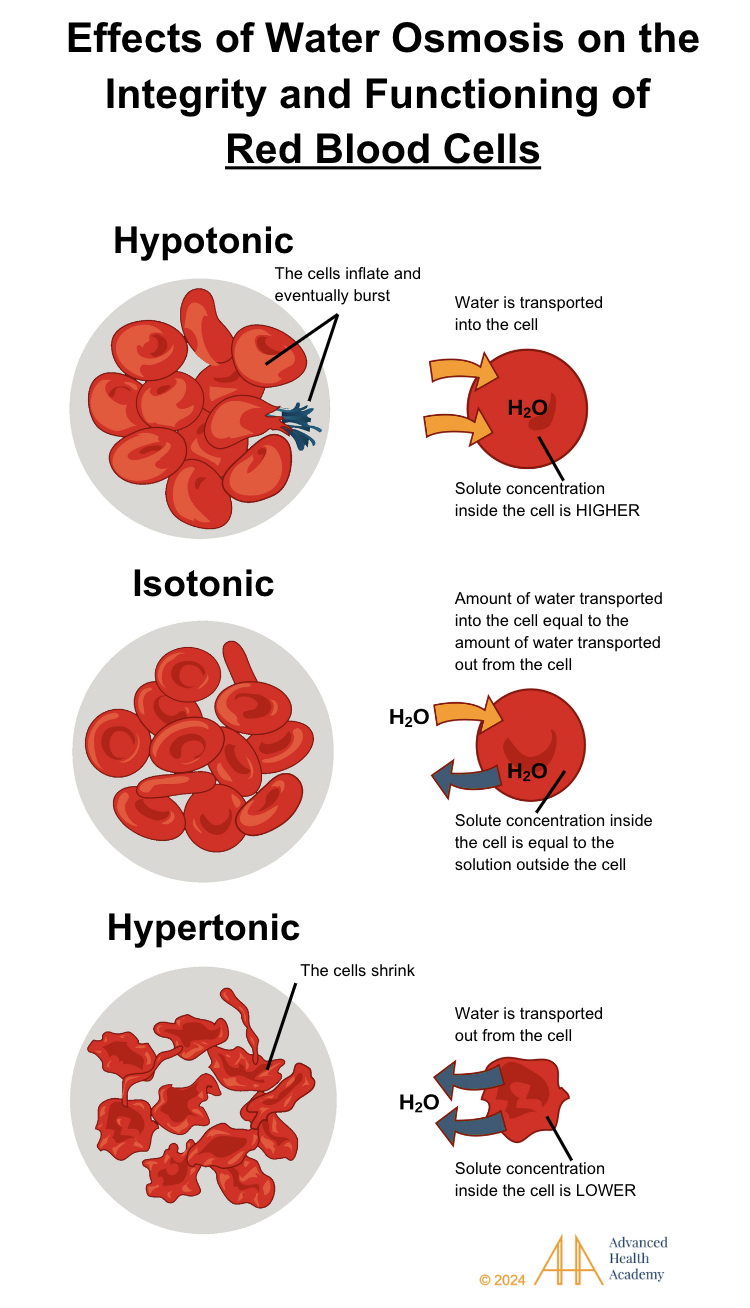
FIGURE 6 Effects of water osmosis on the integrity and functioning of blood cells.
Osmosis moves water based on solute concentration. Hypotonic cells draw water in, isotonic cells balance water movement, and hypertonic cells lose water.
Excess loss of fluid (dehydration) can occur via the following mechanisms:
burns
diarrhea
excessive use of diuretics or laxatives
sweating from strenuous exercise or heat stroke
inadequate water intake
inadequate breast milk consumption in newborns
Excess blood loss is commonly associated with the following69:
Heavy menstrual cycle or chronic inflammation (e.g., inflammatory bowel disease, ulcerative colitis, stomach ulcers, celiac disease, cancer)
Excessive blood loss due to surgery or trauma
Excess donation of blood, e.g., blood draws
ROS can harm microbiota, causing deficiencies in iron, copper, B vitamins, and reduced hemoglobin and RBC production. Chronic dehydration accelerates hypoxia-induced RBC destruction and recruits platelets, WBCs, and smooth muscles to injury sites,. Exposed blood vessel collagen triggers thrombopoietin (TPO) and von Willebrand factor (vWF) production, promoting clotting (thrombus) and angiogenesis. This process, atherosclerosis, restricts blood flow, raises blood pressure, and causes blood to back up into organs like the liver, spleen, heart, and legs, impairing their function.
Accelerated hemolysis overwhelms hemoglobin-scavenging systems and iron storage, often leading to platelet destruction in the spleen.11, Reduced liver function raises undigested proteins, fats, and glucose in the blood, triggering white blood cells (WBCs) to produce antibodies against these antigens. This autoimmune response also targets platelets (APA) to control excess clotting and angiogenesis. High antibody and ROS levels inhibit hematopoietic stem cell conversion in the bone marrow, reducing platelet, WBC, and RBC counts, .
Thrombocytopenia activates megakaryocytes in the lungs and recruits platelets to interact with pathogens (e.g., HIV, hepatitis, diphtheria) and cancer cells, aiding in the uptake of free iron and heme. Platelet activation releases growth factors (GFs) that promote clot formation, guide immune cells, and protect pathogens and tumors from blood flow forces40,48. Excess heme-iron in the blood can suppress T-cells and neutrophils, preventing the destruction of pathogens and tumors. This enables pathogen and tumor growth, excessive clotting, angiogenesis, and reduced bleeding,,,, 57.
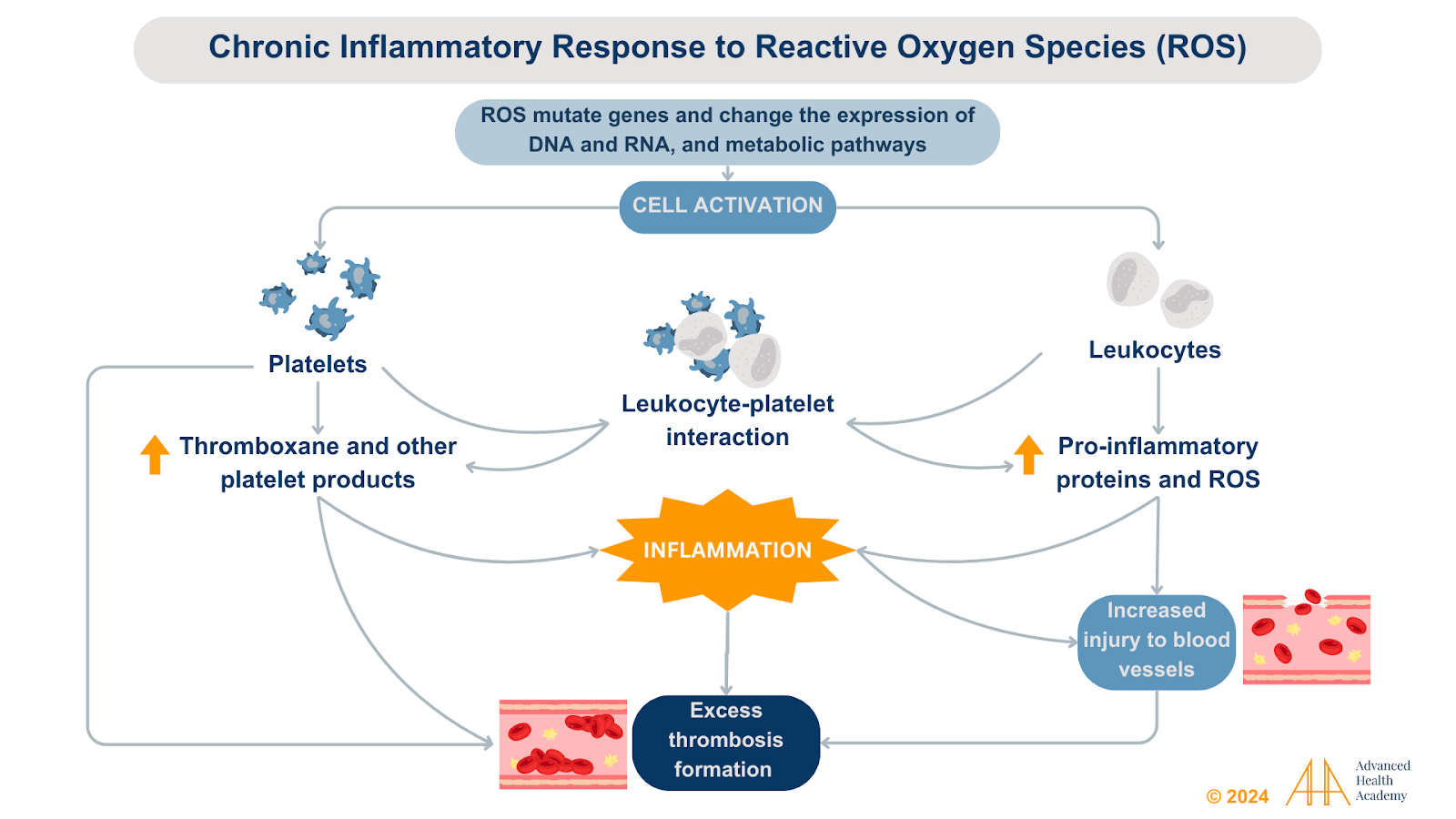
Figure 7. Reactive oxygen species alter various metabolic pathways and enhance the interaction between white blood cells (leukocytes) and platelets. Activated platelets increase clot formation, restrict arterial blood flow, and modulate the immune response.
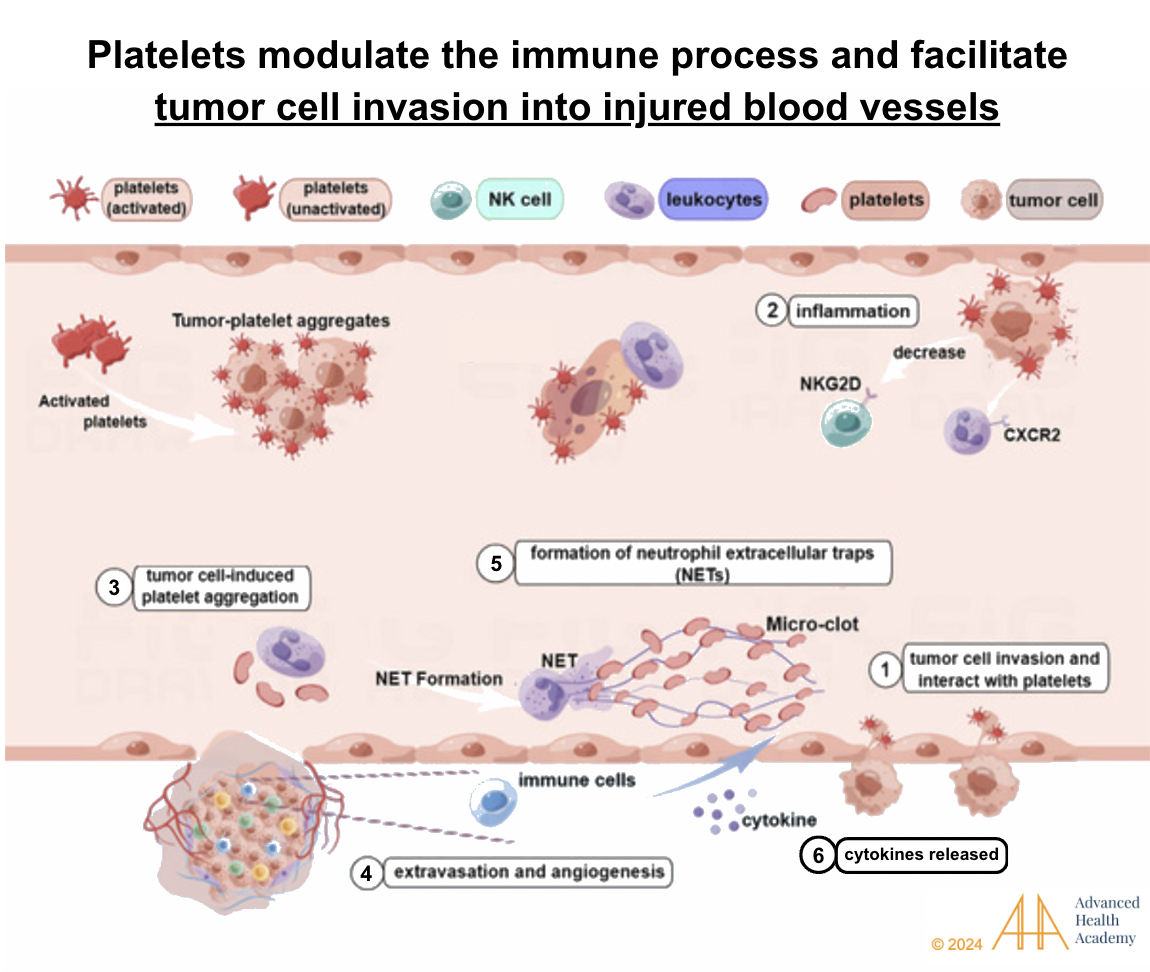
Figure 8: Chronic inflammation facilitates tumor cells and platelet interaction (1 and 2)44. Tumor cells trigger platelet aggregation and support angiogenesis. Activated platelets suppress natural killer (NK) cells, protecting tumors and pathogens while neutrophils stabilize blood vessels and shield tumors. Cytokines from these processes promote tumor growth, migration, and invasion.
Thrombocytosis (High Platelet Count)
Thrombocytosis, a high platelet count, can be primary (essential thrombocythemia) or secondary (reactive).
Primary thrombocytosis is often caused by dehydration, which disrupts gut microbiota, impairing digestion, nutrient absorption, and waste removal. Deficiencies in iron and B vitamins lower hemoglobin, myoglobin, and oxygen delivery (hypoxia). Hypoxia boosts thrombopoietin (TPO) production, driving megakaryocyte formation in bone marrow and releasing inactive platelets into circulation..
The leading cause of secondary thrombocytosis is medications. Secondary thrombocytosis is primarily caused by medications such as aspirin, ADP receptor antagonists, integrin αIIbβ3 inhibitors, NSAIDs, antibiotics, SSRIs, and volume expanders, which alter platelet function and impair clot formation. The second leading cause is vascular interventions or trauma that disrupt platelet activation. , 46
Acquired versus inherited platelet function defects
Platelet-released growth factors can raise ROS levels, damaging cell DNA and expression. Genetic mutations affecting platelet structure and function may occur in utero or after birth1:
Disorders of the adhesive protein receptors
Abnormalities of G protein-coupled receptors
Abnormalities of platelet granules
Defects of signal transduction proteins
Transcription factor defects
Defects of cytoskeletal proteins
Abnormalities of membrane phospholipids
Enhanced platelet fibrinolytic activity
Inherited platelet function defects (IPFDs) are a common but hard-to-diagnose cause of bleeding disorders. They trigger thrombopoietin (TPO) and CFU-meg, increasing myeloid stem cell conversion to megakaryocytes and platelets. Higher TPO and CFU-meg levels correlate with elevated inactive platelet counts11.
Acquired platelet function defects (PFDs) are more common than inherited ones and may occur even with normal platelet counts. Conditions like kidney or liver disease reduce hemoglobin and RBC production while increasing RBC destruction. Cholesterol fills cracks in damaged arteries, triggering white blood cells to release inflammatory proteins. Platelets then form clots, promote new blood vessels, and repair wounds, while smooth muscle cells create plaque, thickening arteries and restricting blood flow (atherosclerosis).
Prevalence and Statistics of Platelet-related Conditions
Thrombocytopenia
Idiopathic Thrombocytopenic Purpura (ITP): an autoimmune disorder where the immune system destroys platelets. It affects about 3.3 per 100,000 adults yearly, more commonly in women, and occurs most often in young adults and older individuals.
Heparin-induced thrombocytopenia (HIT): HIT is a reaction to heparin that lowers platelet count. About 33% of hospitalized U.S. patients receive heparin annually, with HIT occurring in 0.1–5%, especially in surgical patients. Risk starts around day 5 of use, peaking between days 10–14, and is highest with bovine unfractionated heparin (UFH), particularly in female surgical patients.
Bone Marrow Disorders: Bone marrow issues can block stem cells from forming WBCs, RBCs, and platelets, leading to disorders like leukemia and aplastic anemia. In 2021, about 508,796 people in the U.S. had leukemia, while aplastic anemia affects 1–2 people per million yearly.
Thrombocytosis
Primary (Essential Thrombocythemia): a myeloproliferative disorder causing excess platelet production. It affects 0.2–2.5 per 100,000 people annually, with 38–57 cases per 100,000. Risk is highest in people aged 50–70.
Secondary (Reactive Thrombocytosis): Reactive thrombocytosis occurs in response to conditions like infection, chronic inflammation, or cancer. It accounts for 80–90% of thrombocytosis cases and affects 6–15% of hospitalized patients.
Platelet Function Disorders
Inherited Disorders: Conditions like Glanzmann thrombasthenia and Bernard-Soulier syndrome are rare, with fewer than 1 per million incidences.
Acquired Disorders: Medications (e.g., aspirin, clopidogrel) and diseases (e.g., kidney, liver disease) can cause acquired platelet function defects (PFDs). These affect 3–20 per 100,000 people, with 2–10 new cases per 100,000 patient-years. Acquired PFDs are more common but often underreported due to inconsistent definitions and factors.
Conclusion
Platelets support blood vessel integrity, wound healing, and immune defense. Their function depends on gut microbiota, which aids in nutrient absorption and waste removal. Dysbiosis reduces nutrient availability, disrupting protein synthesis for oxygen transport and energy production. Hypoxia damages cells and metabolic pathways, prompting WBCs, platelets, and smooth muscle cells to remove toxins, repair damage, and promote angiogenesis.
Chronic dehydration, dysbiosis, nutrient deficiencies, and hypoxia accelerate red blood cell (RBC) destruction. Excess cholesterol from RBC membranes deposits in injured vessels, leading to clot formation (thrombosis), angiogenesis, and plaque buildup (atherosclerosis). This restricts arterial blood flow, raises blood pressure, and impairs organ function, reducing RBC, WBC, and platelet production while increasing bleeding risk. Megakaryocytes in lung capillaries recruit pathogens and cancer cells, ingest free heme-iron from damaged RBCs, and support clotting and angiogenesis, enabling pathogen and tumor growth.
Platelet count, mean platelet volume, distribution width, and RNA profiles offer insights into various health conditions. Platelets are biomarkers for vascular diseases, autoimmune disorders, infections, and tumors. They store cancer-cell biomolecules that promote tumor growth and spread. Monitoring platelet count aids advanced diagnostics, targeted treatments, and reduces risks linked to conventional therapies for abnormal platelet function.
Source References and Supplemental Research:
Hayward C. Update on diagnostic testing for platelet function disorders. Pathology. 2024;56(S1):S25-S26. doi:10.1016/j.pathol.2023.12.095 [PubMed] [Crosslink]
Gresele P, Falcinelli E, Bury L. Laboratory diagnosis of clinically relevant platelet function disorders. International Journal of Laboratory Hematology. 2018;40(S1):34-45. doi:10.1111/ijlh.12814 [PubMed] [Crosslink]
Mescher, Anthony L. (2018). “Blood”. Junqueira’s Basic Histology: Text and Atlas (15 ed.). McGraw-Hill Education. p. 237. ISBN 9781260026184. Cited by: Cottler-Fox, Michele; Montgomery, Matthew; Theus, John (2009-01-01), Treleaven, Jennifer; Barrett, A John (eds.), “CHAPTER 24 – Collection and processing of marrow and blood hematopoietic stem cells”, Hematopoietic Stem Cell Transplantation in Clinical Practice, Edinburgh: Churchill Livingstone, pp. 249–256, ISBN 978-0-443-10147-2, retrieved 2022-08-09.
Young B, Lowe jo, Stevens A, Heath JW (2006). Wheater’s Functional Histology (5th ed.). Elsevier Limited. ISBN 978-0-443-06850-8.
Jurk K, Kehrel BE. Platelets: Physiology and Biochemistry *. Semin. Thromb. Hemost. 2023;50(05):794–803.
Puri RN, Colman RW, Liberman MA. ADP-lnduced platelet activation. Critical Reviews in Biochemistry and Molecular Biology. 1997;32(6):437-502. doi:10.3109/10409239709082000 [PubMed] [Crosslink]
Badimon L, Padró T, Vilahur G. Atherosclerosis, platelets and thrombosis in acute ischaemic heart disease. European Heart Journal: Acute Cardiovascular Care. 2012;1(1):60-74. doi:10.1177/2048872612441582 [PubMed] [Crosslink]
Periayah MH, Halim AS, Mat Saad AZ. Mechanism Action of Platelets and Crucial Blood Coagulation Pathways in Hemostasis. Int J Hematol Oncol Stem Cell Res. 2017;11(4):319-327. [PubMed] [PMC Full Text]
Holinstat M. Normal platelet function. Cancer Metastasis Rev. 2017;36(2):195-198. doi:10.1007/s10555-017-9677-x [PubMed] [PMC Full Text] [Crosslink]
Rouyez MC, Boucheron C, Gisselbrecht S, Dusanter-Fourt I, Porteu F. Control of thrombopoietin-induced megakaryocytic differentiation by the mitogen-activated protein kinase pathway. Mol Cell Biol. 1997;17:4991-5000 [PubMed] [PMC Full Text]
Ishikawa T, Ichida T, Matsuda Y, Sugitani S, Sugiyama M, Kato T, Miyazaki H, Asakura H. Reduced expression of thrombopoietin is involved in thrombocytopenia in human and rat liver cirrhosis. J Gastroenterol Hepatol. 1998;13:907-913. [PubMed] [Crosslink]
Ishikawa T, Ichida T, Sugahara S, Yamagiwa S, Matsuda Y, Uehara K, Kato T, Miyazaki H, Asakura H. Thrombopoietin receptor (c-Mpl) is constitutively expressed on platelets of patients with liver cirrhosis, and correlates with its disease progression. Hepatol Res. 2002;23:115-121. [PubMed] [Crosslink]
Zhao. Platelet generation from circulating megakaryocytes is triggered in the lung vasculature. BioRXiv (2021) bioRxiv 2021.11.01.466743. doi: 10.21203/rs.3.rs-690639/v1 [BioRXiv Full Text] [Crosslink] Cited by: Gelon L, Fromont L, Lefrançais E. Occurrence and role of lung megakaryocytes in infection and inflammation. Frontiers in Immunology. 2022;13. doi:10.3389/fimmu.2022.1029223 [PubMed] [PMC Full Text] [Crosslink]
Poirault-Chassac S, Nivet-Antoine V, Houvert A, Kauskot A, Lauret E, Lai-Kuen R, et al. Mitochondrial dynamics and reactive oxygen species initiate thrombopoiesis from mature megakaryocytes. Blood Adv (2021) 5(6):1706–18. doi: 10.1182/bloodadvances.2020002847 [PubMed] [PMC Full Text] [Crosslink] Cited by: Gelon L, Fromont L, Lefrançais E. Occurrence and role of lung megakaryocytes in infection and inflammation. Frontiers in Immunology. 2022;13. doi:10.3389/fimmu.2022.1029223 [PubMed] [PMC Full Text] [Crosslink]
Gelon L, Fromont L, Lefrançais E. Occurrence and role of lung megakaryocytes in infection and inflammation. Frontiers in Immunology. 2022;13. doi:10.3389/fimmu.2022.1029223 [PubMed] [PMC Full Text] [Crosslink]
Warkentin TE, Aird WC, Rand JH. Platelet-endothelial interactions: sepsis, HIT, and antiphospholipid syndrome. Hematology Am Soc Hematol Educ Program. 2003;497-519. [PubMed] [Crosslink]
Bunn HF. Hemoglobin I. Structure and function. In: Beck WS, Hematology. Cambridge, MA: MIT Press, 1981;129.
Billett H. Chapter 151: Hemoglobin and Hematocrit. Clinical Methods: The History, Physical and Laboratory Examinations. 3rd Edition. Boston: Butterworths; 1990.
Wallerstein RO. Laboratory evaluation of anemia. West J Med. 1987;146:443. [PubMed] [WJM Full Text]
Singh A, Koritala T, Jialal I. Unconjugated Hyperbilirubinemia. [Updated 2023 Feb 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK549796/# [Full Text]
Weiss G. Iron metabolism in the anemia of chronic disease. Biochim Biophys Acta. 2009;1790:682–693. [PubMed] [Crosslink]
Weiss G, Goodnough LT. Anemia of chronic disease. N Engl J Med. 2005;352:1011–1023. [NEJM Abstract]
Calabrese V, Mancuso C, Calvani M, Rizzarelli E, Butterfield DA, Stella AM. Nitric oxide in the central nervous system: neuroprotection versus neurotoxicity. Nat Rev Neurosci. 2007;8(10):766–775. [PubMed] [Crosslink] [Google Scholar]
Mancuso C, Navarra P, Preziosi P. Roles of nitric oxide, carbon monoxide, and hydrogen sulfide in the regulation of the hypothalamic-pituitary-adrenal axis. J Neurochem. 2010;113(3):563–575. [PubMed] [Crosslink] [Google Scholar]
Rochette L, Cottin Y, Zeller M, Vergely C. Carbon monoxide: mechanisms of action and potential clinical implications. Pharmacol Ther. 2013;137(2):133–152. [PubMed] [Crosslink] [Google Scholar]
Fevery J, Blanckaert N, Heirwegh KP, Préaux AM, Berthelot P. Unconjugated bilirubin and an increased proportion of bilirubin monoconjugates in the bile of patients with Gilbert’s syndrome and Crigler-Najjar disease. J Clin Invest. 1977;60(5):970–979. [PubMed] [PMC Full Text] [Crosslink] [Google Scholar]
Dludla P.V., Joubert E., Muller C.J.F., Louw J., Johnson R. Hyperglycemia-induced oxidative stress and heart disease-cardioprotective effects of rooibos flavonoids and phenylpyruvic acid-2-O-beta-D-glucoside. Nutr. Metab. 2017;14:45. doi: 10.1186/s12986-017-0200-8. [PubMed] [PMC Full Text] [Crosslink] [Google Scholar]. Cited by: Žiberna L, Jenko-Pražnikar Z, Petelin A. Serum Bilirubin Levels in Overweight and Obese Individuals: The Importance of Anti-Inflammatory and Antioxidant Responses. Antioxidants (Basel). 2021;10(9):1352. Published 2021 Aug 26. doi:10.3390/antiox10091352 [PubMed] [PMC Full Text]
Han C.Y. Roles of Reactive Oxygen Species on Insulin Resistance in Adipose Tissue. Diabetes Metab. J. 2016;40:272–279. doi: 10.4093/dmj.2016.40.4.272. [PubMed] [PMC Full Text][Crosslink] [Google Scholar]. Cited by: Žiberna L, Jenko-Pražnikar Z, Petelin A. Serum Bilirubin Levels in Overweight and Obese Individuals: The Importance of Anti-Inflammatory and Antioxidant Responses. Antioxidants (Basel). 2021;10(9):1352. Published 2021 Aug 26. doi:10.3390/antiox10091352 [PubMed] [PMC Full Text]
Boskabadi H, Rakhshanizadeh F. Neonatal hypernatremic dehydration and thrombocytopenia: Its prevalence and relationship with prognosis. Iranian Journal of Pediatrics. 2018;28(4). doi:10.5812/ijp.65742 [Crosslink]
Martin TG 3rd, Somberg KA, Meng YG, Cohen RL, Heid CA, de Sauvage FJ, Shuman MA. Thrombopoietin levels in patients with cirrhosis before and after orthotopic liver transplantation. Ann Intern Med. 1997;127:285-288. [PubMed] [Crosslink]
Panzer S, Seel E. Is there an increased frequency of autoimmune thrombocytopenia in hepatitis C infection? Wien Med Wochenschr. 2003;153:417-420. [PubMed] [Crosslink]
Misiani R, Bellavita P, Fenili D, Borelli G, Marchesi D, Massazza M, Vendramin G, Comotti B, Tanzi E, Scudeller G. Hepatitis C virus infection in patients with essential mixed cryoglobulinemia. Ann Intern Med. 1992;117:573-577. [PubMed] [PMC Full Text]
Sritharan M (July 2006). “Iron and bacterial virulence”. Indian J Med Microbiol. 24 (3): 163–4. doi:10.1016/S0255-0857(21)02343-4. PMID 16912433. [Crosslink]
Landolfi R, Di Gennaro L. Pathophysiology of thrombosis in myeloproliferative neoplasms. Haematologica. 2011;96(2):183-186. doi:10.3324/haematol.2010.038299 [PubMed] [PMC Full Text] [Crosslink]
Liu Y, Li P, Lu J, Xiong W, Oger J, Tetzlaff W, Cynader M. Bilirubin possesses powerful immunomodulatory activity and suppresses experimental autoimmune encephalomyelitis. J Immunol 181: 1887–1897, 2008. doi: 10.4049/jimmunol.181.3.1887. [PubMed] [Crosslink] [Google Scholar]. Cited by: Creeden JF, Gordon DM, Stec DE, Hinds TD Jr. Bilirubin as a metabolic hormone: the physiological relevance of low levels. Am J Physiol Endocrinol Metab. 2021;320(2):E191-E207. doi:10.1152/ajpendo.00405.2020 [Crosslink]
Weinberger B, Archer FE, Kathiravan S, Hirsch DS, Kleinfeld AM, Vetrano AM, Hegyi T. Effects of bilirubin on neutrophil responses in newborn infants. Neonatology 103: 105–111, 2013. doi: 10.1159/000343097. [PMC Full Text] [PubMed] [Crosslink] [Google Scholar]. Cited by: Creeden JF, Gordon DM, Stec DE, Hinds TD Jr. Bilirubin as a metabolic hormone: the physiological relevance of low levels. Am J Physiol Endocrinol Metab. 2021;320(2):E191-E207. doi:10.1152/ajpendo.00405.2020 [Crosslink]
McPhee F, Caldera PS, Bemis GW, McDonagh AF, Kuntz ID, Craik CS. Bile pigments as HIV-1 protease inhibitors and their effects on HIV-1 viral maturation and infectivity in vitro. Biochem J 320: 681–686, 1996. doi: 10.1042/bj3200681. [PMC Full Text] [PubMed] [Crosslink] [Google Scholar]. Cited by: Creeden JF, Gordon DM, Stec DE, Hinds TD Jr. Bilirubin as a metabolic hormone: the physiological relevance of low levels. Am J Physiol Endocrinol Metab. 2021;320(2):E191-E207. doi:10.1152/ajpendo.00405.2020 [Crosslink]
Zhu Z, Wilson AT, Luxon BA, Brown KE, Mathahs MM, Bandyopadhyay S, McCaffrey AP, Schmidt WN. Biliverdin inhibits hepatitis C virus nonstructural 3/4A protease activity: mechanism for the antiviral effects of heme oxygenase? Hepatology 52: 1897–1905, 2010. doi: 10.1002/hep.23921. [PMC Full Text] [PubMed] [Crosslink] [Google Scholar]. Cited by: Creeden JF, Gordon DM, Stec DE, Hinds TD Jr. Bilirubin as a metabolic hormone: the physiological relevance of low levels. Am J Physiol Endocrinol Metab. 2021;320(2):E191-E207. doi:10.1152/ajpendo.00405.2020 [Crosslink]
Castro-Garcia FP, Corral-Jara KF, Escobedo-Melendez G, Sandoval-Hernandez MA, Rosenstein Y, Roman S, Panduro A, Fierro NA. Conjugated bilirubin affects cytokine profiles in hepatitis A virus infection by modulating function of signal transducer and activator of transcription factors. Immunology 143: 578–587, 2014. doi: 10.1111/imm.12336. [PMC Full Text] [PubMed] [Crosslink] [Google Scholar]. Cited by: Creeden JF, Gordon DM, Stec DE, Hinds TD Jr. Bilirubin as a metabolic hormone: the physiological relevance of low levels. Am J Physiol Endocrinol Metab. 2021;320(2):E191-E207. doi:10.1152/ajpendo.00405.2020 [Crosslink]
Garcia, J., Mankin, P., Gnanamony, M. et al. Evaluation of angiogenic signaling molecules associated with reactive thrombocytosis in an iron-deficient rat model. Pediatr. Res. https://doi.org/10.1038/s41390-020-01318-0 (2021) [PR Full Text] [Crosslink]
Brennan Y, Levade M, Ward CM. Acquired platelet function disorders. Thrombosis Research. 2020;196:561-568. doi:10.1016/j.thromres.2019.06.009 [PubMed] [Crosslink]
Scharf RE. Acquired disorders of platelet function. Platelets. Published online 2019:905-920. doi:10.1016/b978-0-12-813456-6.00049-7 [Crosslink]
Gresele P, Falcinelli E, Bury L. Laboratory diagnosis of clinically relevant platelet function disorders. International Journal of Laboratory Hematology. 2018;40(S1):34-45. doi:10.1111/ijlh.12814 [PubMed] [Crosslink]
Liao K, Zhang X, Liu J, et al. The role of platelets in the regulation of tumor growth and metastasis: the mechanisms and targeted therapy. MedComm (2020). 2023;4(5):e350. Published 2023 Sep 14. doi:10.1002/mco2.350 [PubMed] [PMC Full Text] [Crosslink]
Kohli R, Chaturvedi S. Epidemiology and clinical manifestations of immune thrombocytopenia. Hämostaseologie. 2019;39(03):238-249. doi:10.1055/s-0039-1683416 [PubMed] [Crosslink]
Alhanshani AA. Heparin induced thrombocytopenia – pathophysiology, diagnosis and treatment: A narrative review. International Journal of General Medicine. 2023;Volume 16:3947-3953. doi:10.2147/ijgm.s420327 [PubMed] [PMC Full Text] [Crosslink]
Zinkovsky DA, Antonopoulos MS. Heparin-induced thrombocytopenia: overview and treatment. P T. 2008;33(11):642-651.[PubMed] [PMC Full Text]
Leukemia – Cancer Stat Facts. SEER. Accessed July 3, 2024.
Accurso V, Santoro M, Mancuso S, et al. The Essential Thrombocythemia in 2020: What We Know and Where We Still Have to Dig Deep. Clin Med Insights Blood Disord. 2020;13:2634853520978210. Published 2020 Dec 28. doi:10.1177/2634853520978210 [PubMed] [PMC Full Text] [Crosslink]
Mohan G, Malayala SV, Mehta P, Balla M. A Comprehensive Review of Congenital Platelet Disorders, Thrombocytopenias and Thrombocytopathies. Cureus. 2020;12(10):e11275. Published 2020 Oct 31. doi:10.7759/cureus.11275 [PubMed] [PMC Full Text] [Crosslink]
Atherosclerosis: Symptoms. National Heart Lung and Blood Institute. Accessed July 15, 2024. https://www.nhlbi.nih.gov/health/atherosclerosis/symptoms. [NIH]
Yi SL, Buicko Lopez JL. Splenectomy. [Updated 2024 May 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan.
Gallo P, Terracciani F, Di Pasquale G, Esposito M, Picardi A, Vespasiani-Gentilucci U. Thrombocytopenia in chronic liver disease: Physiopathology and new therapeutic strategies before invasive procedures. World J Gastroenterol 2022; 28(30): 4061-4074 [PubMed] [PMC Full Text] [Crosslink]
Beutler E., Bothwell T.H., Charlton R.W., Motulsky A.G. Hereditary Hemochromatosis. The McGraw-Hill Companies; New York, NY, USA: 2006. [Crosslink] [Google Scholar]. Cited by: Hooda J, Shah A, Zhang L. Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients. 2014;6(3):1080-1102. Published 2014 Mar 13. doi:10.3390/nu6031080 [PubMed] [PMC Full Text] [Crosslink]
Schwartz S., Ellefson M. Quantitative fecal recovery of ingested hemoglobin-heme in blood: Comparisons by hemoquant assay with ingested meat and fish. Gastroenterology. 1985;89:192–196. [PubMed] [Crosslink] [Google Scholar]. Cited by: Hooda J, Shah A, Zhang L. Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients. 2014;6(3):1080-1102. Published 2014 Mar 13. doi:10.3390/nu6031080 [PubMed] [PMC Full Text] [Crosslink]
Briat J.F., Curie C., Gaymard F. Iron utilization and metabolism in plants. Curr. Opin. Plant Biol. 2007;10:276–282. doi: 10.1016/j.pbi.2007.04.003. [PubMed] [Crosslink] [Google Scholar]
Raffin S.B., Woo C.H., Roost K.T., Price D.C., Schmid R. Intestinal absorption of hemoglobin iron-heme cleavage by mucosal heme oxygenase. J. Clin. Investig. 1974;54:1344–1352. [PMC Full Text] [PubMed] [Crosslink] [Google Scholar]. Cited by: Hooda J, Shah A, Zhang L. Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients. 2014;6(3):1080-1102. Published 2014 Mar 13. doi:10.3390/nu6031080 [PubMed] [PMC Full Text] [Crosslink]
West A.R., Oates P.S. Mechanisms of heme iron absorption: Current questions and controversies. World J. Gastroenterol. 2008;14:4101–4110. doi: 10.3748/wjg.14.4101. [PMC Full Text] [PubMed] [Crosslink] [Google Scholar]. Cited by: Hooda J, Shah A, Zhang L. Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients. 2014;6(3):1080-1102. Published 2014 Mar 13. doi:10.3390/nu6031080 [PubMed] [PMC Full Text] [Crosslink]
Conrad M.E., Umbreit J.N. Iron absorption and transport—An update. Am. J. Hematol. 2000;64:287–298. doi: 10.1002/1096-8652(200008)64:4<287::AID-AJH9>3.0.CO;2-L. [PubMed] [Crosslink] [Google Scholar]. Cited by: Hooda J, Shah A, Zhang L. Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients. 2014;6(3):1080-1102. Published 2014 Mar 13. doi:10.3390/nu6031080
Fuqua B.K., Vulpe C.D., Anderson G.J. Intestinal iron absorption. J. Trace Elem. Med. Biol. 2012;26:115–119. doi: 10.1016/j.jtemb.2012.03.015. [PubMed] [Crosslink] [Google Scholar]. Cited by: Hooda J, Shah A, Zhang L. Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients. 2014;6(3):1080-1102. Published 2014 Mar 13. doi:10.3390/nu6031080 [PubMed] [PMC Full Text] [Crosslink]
Jacobs A. Availability and absorption of dietary iron. Proc. R. Soc. Med. 1970;63:1215–1216. [PMC Full Text] [PubMed] [Google Scholar]. Cited by: Hooda J, Shah A, Zhang L. Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients. 2014;6(3):1080-1102. Published 2014 Mar 13. doi:10.3390/nu6031080 [PubMed] [PMC Full Text] [Crosslink]
Vaghefi N., Nedjaoum F., Guillochon D., Bureau F., Arhan P., Bougle D. Influence of the extent of hemoglobin hydrolysis on the digestive absorption of heme iron. An in vitro study. J. Agric. Food Chem. 2002;50:4969–4973. doi: 10.1021/jf0109165. [PubMed] [Crosslink] [Google Scholar]. Cited by: Hooda J, Shah A, Zhang L. Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients. 2014;6(3):1080-1102. Published 2014 Mar 13. doi:10.3390/nu6031080 [PubMed] [PMC Full Text] [Crosslink]
Han O. Molecular mechanism of intestinal iron absorption. Metallomics. 2011;3:103–109. doi: 10.1039/c0mt00043d. [PubMed] [Crosslink] [Google Scholar]. Cited by: Hooda J, Shah A, Zhang L. Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients. 2014;6(3):1080-1102. Published 2014 Mar 13. doi:10.3390/nu6031080 [PubMed] [PMC Full Text] [Crosslink]
Krishnamurthy P., Xie T., Schuetz J.D. The role of transporters in cellular heme and porphyrin homeostasis. Pharmacol. Ther. 2007;114:345–358. [PubMed] [Crosslink] [Google Scholar]. Cited by: Hooda J, Shah A, Zhang L. Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients. 2014;6(3):1080-1102. Published 2014 Mar 13. doi:10.3390/nu6031080 [PubMed] [PMC Full Text] [Crosslink]
Hooda J., Cadinu D., Alam M.M., Shah A., Cao T.M., Sullivan L.A., Brekken R., Zhang L. Enhanced heme function and mitochondrial respiration promote the progression of lung cancer cells. PLoS One. 2013;8:e63402. [PMC Full Text] [PubMed] [Crosslink] [Google Scholar]. Hooda J, Shah A, Zhang L. Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients. 2014;6(3):1080-1102. Published 2014 Mar 13. doi:10.3390/nu6031080 [PubMed] [PMC Full Text] [Crosslink]
Hooda J, Shah A, Zhang L. Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients. 2014;6(3):1080-1102. Published 2014 Mar 13. doi:10.3390/nu6031080 [PubMed] [PMC Full Text] [Crosslink]
Yi J, Thomas LM, Musayev FN, Safo MK, Richter-Addo GB. Crystallographic trapping of heme loss intermediates during the nitrite-induced degradation of human hemoglobin. Biochemistry. 2011;50(39):8323-8332. doi:10.1021/bi2009322 and RCSB PDB [PubMed] [PMC Full Text] [Crosslink]
Hubbard SR, Hendrickson WA, Lambright DG, Boxer SG. X-ray crystal structure of a recombinant human myoglobin mutant at 2.8 A resolution. J Mol Biol. 1990;213(2):215-218. doi:10.1016/S0022-2836(05)80181-0 and RCSB PDB [PubMed] [Crosslink]
Jiang R., Ma J., Ascherio A., Stampfer M.J., Willett W.C., Hu F.B. Dietary iron intake and blood donations in relation to risk of type 2 diabetes in men: A prospective cohort study. Am. J. Clin. Nutr. 2004;79:70–75. [PubMed] [Google Scholar] [Crosslink] Cited by: Hooda J, Shah A, Zhang L. Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients. 2014;6(3):1080-1102. Published 2014 Mar 13. doi:10.3390/nu6031080 [PubMed] [PMC Full Text] [Crosslink]
Zhao Z., Li S., Liu G., Yan F., Ma X., Huang Z., Tian H. Body iron stores and heme-iron intake in relation to risk of type 2 diabetes: A systematic review and meta-analysis. PLoS One. 2012;7:e41641. [PMC Full Text] [PubMed] [Crosslink] [Google Scholar] Cited by: Hooda J, Shah A, Zhang L. Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients. 2014;6(3):1080-1102. Published 2014 Mar 13. doi:10.3390/nu6031080 [PubMed] [PMC Full Text] [Crosslink]
Jehn M.L., Guallar E., Clark J.M., Couper D., Duncan B.B., Ballantyne C.M., Hoogeveen R.C., Harris Z.L., Pankow J.S. A prospective study of plasma ferritin level and incident diabetes: The Atherosclerosis Risk in Communities (ARIC) Study. Am. J. Epidemiol. 2007;165:1047–1054. doi: 10.1093/aje/kwk093. [PubMed] [Crosslink] [Google Scholar] Cited by: Hooda J, Shah A, Zhang L. Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients. 2014;6(3):1080-1102. Published 2014 Mar 13. doi:10.3390/nu6031080 [PubMed] [PMC Full Text] [Crosslink]
Qiu C., Zhang C., Gelaye B., Enquobahrie D.A., Frederick I.O., Williams M.A. Gestational diabetes mellitus in relation to maternal dietary heme iron and nonheme iron intake. Diabetes Care. 2011;34:1564–1569. doi: 10.2337/dc11-0135. [PubMed] [PMC Full Text] [Crosslink] [Google Scholar] Cited by: Hooda J, Shah A, Zhang L. Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients. 2014;6(3):1080-1102. Published 2014 Mar 13. doi:10.3390/nu6031080 [PubMed] [PMC Full Text] [Crosslink]
Rajpathak S., Ma J., Manson J., Willett W.C., Hu F.B. Iron intake and the risk of type 2 diabetes in women: A Prospective Cohort Study. Diabetes Care. 2006;29:1370–1376. doi: 10.2337/dc06-0119. [PubMed] [Crosslink] [Google Scholar] Cited by: Hooda J, Shah A, Zhang L. Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients. 2014;6(3):1080-1102. Published 2014 Mar 13. doi:10.3390/nu6031080 [PubMed] [PMC Full Text] [Crosslink]
Ascherio A., Hennekens C.H., Buring J.E., Master C., Stampfer M.J., Willett W.C. Trans-fatty acids intake and risk of myocardial infarction. Circulation. 1994;89:94–101. doi: 10.1161/01.CIR.89.1.94. [PubMed] [Crosslink] [Google Scholar] Cited by: Hooda J, Shah A, Zhang L. Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients. 2014;6(3):1080-1102. Published 2014 Mar 13. doi:10.3390/nu6031080 [PubMed] [PMC Full Text] [Crosslink]
Snowdon D.A., Phillips R.L., Fraser G.E. Meat consumption and fatal ischemic heart disease. Prev. Med. 1984;13:490–500. doi: 10.1016/0091-7435(84)90017-3. [PubMed] [Crosslink] [Google Scholar] Cited by: Hooda J, Shah A, Zhang L. Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients. 2014;6(3):1080-1102. Published 2014 Mar 13. doi:10.3390/nu6031080 [PubMed] [PMC Full Text] [Crosslink]
Hernáez Á, Lassale C, Castro-Barquero S, et al. Mediterranean Diet Maintained Platelet Count within a Healthy Range and Decreased Thrombocytopenia-Related Mortality Risk: A Randomized Controlled Trial. Nutrients. 2021;13(2):559. Published 2021 Feb 8. doi:10.3390/nu13020559 [PubMed] [PMC Full Text] [Crosslink]
Amin I. “dietary factors influencing platelet counts: Knowledge to improve concentration for platelet-rich plasma injections.” Annals of Reviews & Research. 2023;10(2). doi:10.19080/arr.2023.10.555782 [ARR Full Text] [Crosslink]
Lange M, Nadkarni D, Martin L, Newberry C, Kumar S, Kushner T. Intermittent fasting improves hepatic end points in nonalcoholic fatty liver disease: A systematic review and meta-analysis. Hepatol Commun. 2023;7(8):e0212. Published 2023 Aug 3. doi:10.1097/HC9.0000000000000212 [PubMed] [PMC Full Text] [Crosslink]
Ramsay DJ. Homeostatic control of water balance. In: Arnaud MJ, editor. Hydration Throughout Life. Montrouge: John Libbey Eurotext; 1998. pp. 9–18.
Hom J, Dulmovits B M, Mohandas N, Blanc L. The erythroblastic island as an emerging paradigm in the anemia of inflammation. Immunol Res. 2015 Dec; 63(0): 75–89. [PubMed] [PMC Full Text] [Crosslink]
Silczuk A, Habrat B. Alcohol-induced thrombocytopenia: Current review. Alcohol. 2020;86:9-16. doi:10.1016/j.alcohol.2020.02.166 [PubMed] [Crosslink]
Barale C, Melchionda E, Tempesta G, Morotti A, Russo I. Impact of physical exercise on platelets: Focus on its effects in metabolic chronic diseases. Antioxidants. 2023;12(8):1609. doi:10.3390/antiox12081609 [PubMed] [PMC Full Text] [Crosslink]
Bergmann K, Bergmann OJ. An unusual case of extreme thrombocytosis caused by iron deficiency. BMJ Case Reports. 2020;13(1). doi:10.1136/bcr-2019-231833 [PubMed] [PMC Full Text] [Crosslink]
Li X, Li N, Zhao G, Wang X. Effect of iron supplementation on platelet count in adult patients with iron deficiency anemia. Platelets. 2022;33(8):1214-1219. doi:10.1080/09537104.2022.2091772 [PubMed] [Crosslink]
Murray-Kolbe LE, Beard J. Iron. In: Coates PM, Betz JM, Blackman MR, et al., eds. Encyclopedia of Dietary Supplements. 2nd ed. London and New York: Informa Healthcare; 2010:432-8.
Manoguerra AS, Erdman AR, Booze LL, Christianson G, Wax PM, Scharman EJ, et al. Iron ingestion: an evidence-based consensus guideline for out-of-hospital management. Clin Toxicol (Phila) 2005;43:553-70. [PubMed] [Crosslink]
Institute of Medicine. Food and Nutrition Board. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc : a Report of the Panel on Micronutrients. Washington, DC: National Academy Press; 2001.
Hurrell R, Egli I. Iron bioavailability and dietary reference values. Am J Clin Nutr 2010;91:1461S-7S. [PubMed] [Elsevier]
Lonnerdal B. Calcium and iron absorption–mechanisms and public health relevance. Int J Vitam Nutr Res 2010;80:293-9. [PubMed] [Crosslink]
Lynch SR. The effect of calcium on iron absorption. Nutr Res Rev 2000;13:141-58. [PubMed]
Hanna M, Jaqua E, Nguyen V, Clay J. B Vitamins: Functions and Uses in Medicine. Perm J. 2022;26(2):89-97. doi:10.7812/TPP/21.204 [PubMed] [PMC Full Text] [Crosslink]
Abosheaishaa H, Nassar M, Ghallab M, et al. Pernicious Anemia and Vitamin B12 Deficiency Presenting As Pseudothrombotic Microangiopathy and Developing Secondary Thrombocytopenia After Treatment: A Case Report. Cureus. 2022;14(12):e32095. Published 2022 Dec 1. doi:10.7759/cureus.32095 [PubMed] [PMC Full Text] [Crosslink]
Office of Dietary Supplements – Vitamin B6. NIH Office of Dietary Supplements. Accessed July 4, 2024.
U.S. Food and Drug Administration. Guidance for Industry: A Food Labeling Guide external link disclaimer (14. Appendix F: Calculate the Percent Daily Value for the Appropriate Nutrients). 2013.
Office of Dietary Supplements – Folate. NIH Office of Dietary Supplements. Accessed July 4, 2024.
S. J. Moore, A. D. Lawrence, R. Biedendieck, E. Deery, S. Frank, M. J. Howard, S. E. J. Rigby, M. J. Warren. Elucidation of the anaerobic pathway for the corrin component of cobalamin (vitamin B12). Proceedings of the National Academy of Sciences, 2013; DOI: 10.1073/pnas.1308098110 [PubMed] [PMC Full Text] Crosslink]
Watanabe F, Bito T. Vitamin B12 sources and microbial interaction. Exp Biol Med (Maywood). 2018 Jan;243(2):148-158. doi: 10.1177/1535370217746612. Epub 2017 Dec 7. PMID: 29216732; PMCID: PMC5788147. [PubMed] [PMC Full Text] [Crosslink]
Jones L. Vitamin B12 for Vegans & Vegetarians: Best Natural Sources. Fresh N Lean. June 1, 2023. Accessed July 4, 2024.