Sodium: Diagnostic Significance and Clinical Insights
Authors: Dr. Payal Bhandari, M.D., Hailey Chin
Contributors: Vivi Chador
Key Insights
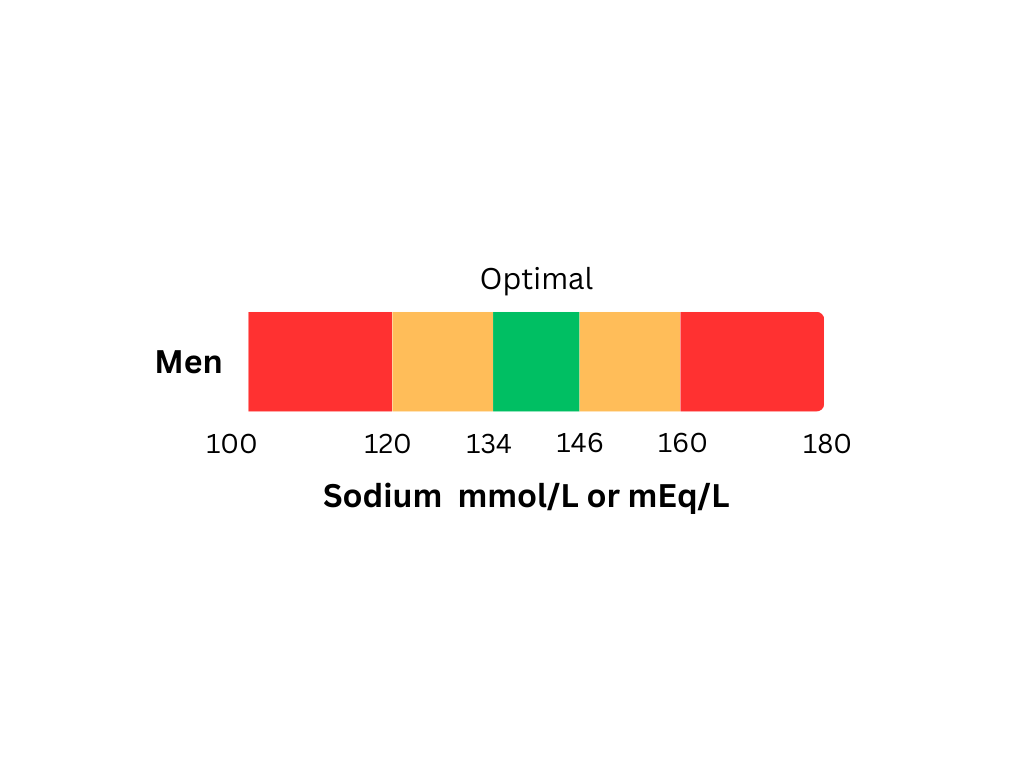
Sodium (Na+) is important for many body functions, including fluid balance, blood pressure, nerve signals, and muscle movement. Testing sodium levels in the blood can help identify problems with organs that might not be working properly. Abnormal sodium levels can cause symptoms like dizziness, headaches, muscle cramps, swelling, confusion, and heart rhythm problems. Sodium tests are useful for managing conditions like high blood pressure, organ dysfunction, and failure (such as heart, kidney, and adrenal problems). Regular sodium testing can also guide changes in diet, lifestyle, and medication to prevent serious health issues and improve overall well-being.
What is Sodium?
Sodium is an important mineral that helps with nerve function, muscle movement, and keeping fluid levels balanced. About 95% of sodium is in the blood and plasma, while the rest is in bones, skin, and muscles . The sodium-potassium (Na+/K+) pump helps move other ions, like potassium and calcium, in and out of cells. It exchanges sodium outside the cell for potassium inside, helping maintain the right balance of ions. This balance is key for cells to get energy and work properly.
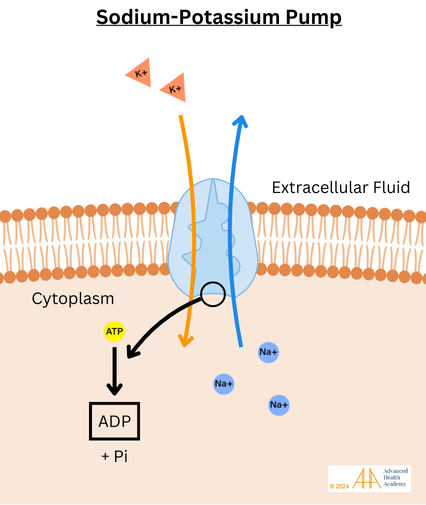
Figure 1: The sodium-potassium pump (Na+/K+-ATPase) is an important protein in cells that helps maintain a balance of sodium (Na+) and potassium (K+) ions. It uses energy from ATP to move three sodium ions out of the cell and two potassium ions into the cell. This process helps control important functions like nerve signaling and muscle movement.
Sodium ions are essential for nerve signals in the brain and body. When a nerve impulse moves along a neuron, sodium ions enter the cell, helping to carry the signal. This process is vital for sensory perception, motor control, and brain functions.
Sodium is also important for muscle movement. It helps muscles contract and relax by working with calcium ions. Maintaining the right sodium levels is crucial for muscle function. Too much or too little sodium can lead to muscle weakness, cramps, and numbness.
In the kidneys, sodium helps control fluid balance and blood pressure. It ensures cells stay hydrated, nutrients are absorbed, and waste is removed. Proper sodium levels also help blood flow, which is necessary for oxygen delivery to tissues. Without enough oxygen, the kidneys struggle to maintain fluid and electrolyte balance, which can lead to dehydration and imbalances in sodium, magnesium, calcium, and potassium. Therefore, maintaining healthy sodium levels is important to prevent health issues like high blood pressure, low energy, and dehydration.
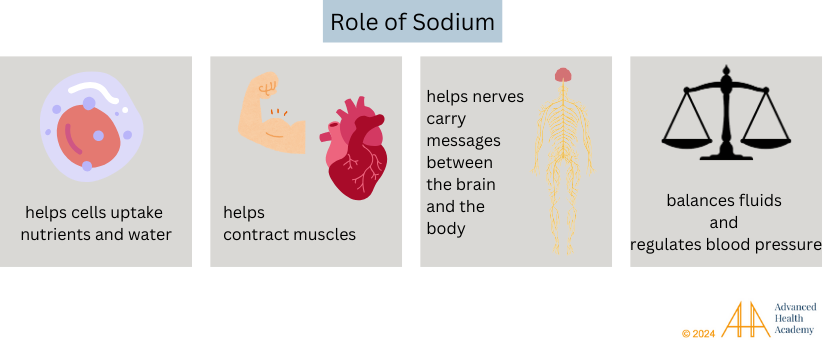
Figure 2: Sodium helps control fluid balance, blood pressure, and nerve signals. It’s important for muscle movement and keeps organs working properly. Sodium also helps balance acids in the body. Keeping the right sodium level is essential for health.
Regulation of Sodium Levels in the Body
Sodium levels in the body are controlled by hormones and organs like the kidneys and small intestines. To keep sodium levels in balance, the body adjusts how much sodium is removed through urine, sweat, and stool.
Most sodium comes from food, especially table salt, processed foods, and some vegetables and meats. After eating, sodium is absorbed into the bloodstream, where it helps control fluid balance and blood pressure. The kidneys filter about 552,000 mg of sodium daily, reabsorbing 99% of it and excreting about 5,520 milligrams (mg) in urine.
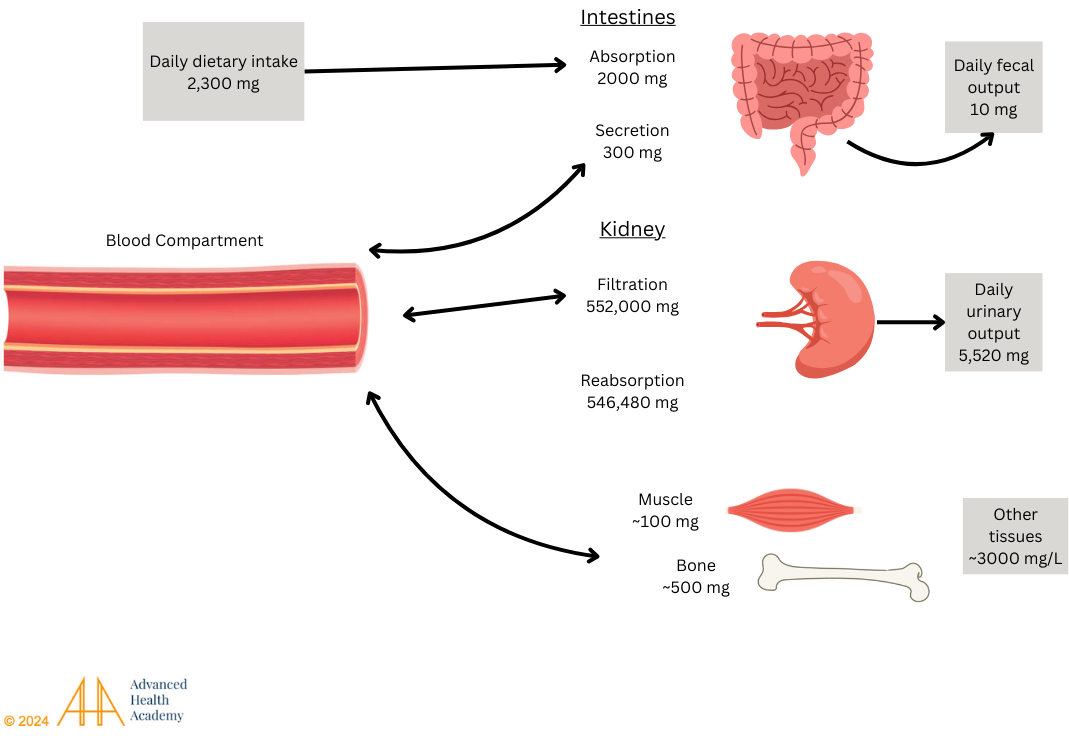
Figure 3: Sodium absorption primarily occurs in the small intestine. It is then released into the bloodstream, filtered by the kidneys, and reabsorbed. Most unused sodium is excreted in the urine, with a small percentage stored in the bones and skeletal muscles.
The renin-angiotensin-aldosterone system (RAAS) helps control sodium levels. When sodium or blood pressure drops, the kidneys release renin, which creates angiotensin II. This triggers aldosterone, which helps the kidneys retain sodium and remove potassium. When sodium is too high or blood pressure rises, the heart releases atrial natriuretic peptide (ANP), telling the kidneys to remove excess sodium and water. Imbalances in sodium can lead to high blood pressure or too much sodium, causing serious health problems like blood vessel inflammation and nerve damage. Proper sodium control is important for overall health.
Clinical Significance of High Blood Sodium Levels
Hypernatremia is when the sodium levels in the blood are too high. It usually happens when the body loses more water than it takes in (dehydration) due to not drinking enough, losing too much water, or consuming too much salt. Dehydration pulls water out of cells, causing them to shrink. This makes the cells less able to function and more prone to damage. The brain detects this shrinkage through two sensors: one controls thirst, and the other regulates urine by releasing a hormone called vasopressin, which causes the body to produce less, more concentrated urine.

Figure 4: Effects of water osmosis on the integrity and function of blood cells. Water osmosis is the transportation of water through a cell that is determined by the cell’s solute concentration. Hypotonic cells have a higher solute concentration inside the cell than outside of the cell causing more water to be transported inside of the cell. Isotonic cells have the same solute concentration inside the cell and outside the cell causing water to be transported into and out from the cell equally. Hypertonic cells have less solute concentration inside the cell causing the cell to transport water out of the cell.
Dehydration can happen due to:
Burns
Diarrhea
Overuse of diuretics or laxatives
Sweating from intense exercise or heat stroke
Not drinking enough water
Insufficient breast milk intake in newborns
Excessive blood loss can be caused by:
Slow blood loss from heavy periods or diseases like inflammatory bowel disease, ulcers, celiac disease, or certain cancers
Sudden blood loss from surgery or trauma
Frequent blood donations, such as blood draws
Dehydration affects fluid levels in cells and raises sodium levels outside cells. To adjust, the kidneys release renin, which triggers the adrenal glands to produce aldosterone. Aldosterone helps the body retain sodium and get rid of potassium through urine, balancing blood flow and pressure. The heart also increases atrial natriuretic peptide to help the kidneys excrete sodium. Over time, chronic dehydration can cause problems with sodium levels, making it harder for the body to maintain essential functions.
Dysbiosis and Atherosclerosis-Induced Vascular Inflammation
The plasma in our blood is mostly water (90%). Hypernatremia, which is too much sodium in the blood, reduces blood flow to the digestive system and kidneys. This can harm healthy gut bacteria, reduce digestion, nutrient absorption, and waste removal.
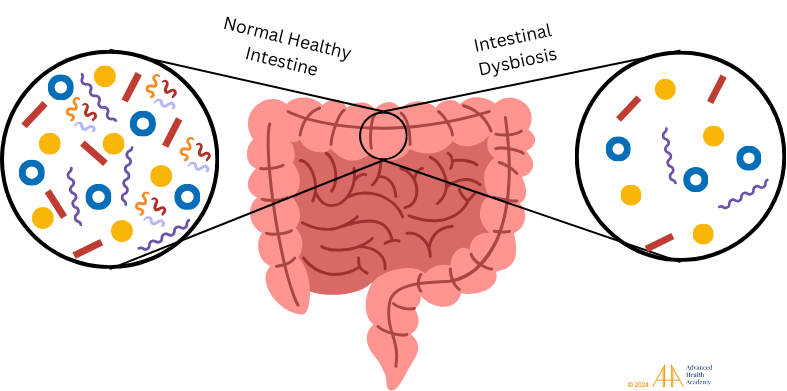
Figure 5: A healthy gut microbiota is key to digestion, nutrient absorption, and waste removal. Dysbiosis happens when healthy bacteria decrease, disrupting metabolism, reducing energy, and causing inflammation. This leads to more harmful pathogens, proteins, and bad cholesterol in the blood.
These changes also prevent the production of important substances like digestive enzymes and hydrochloric acid (HCl) in the stomach. Without enough of these, it’s harder to break down proteins into amino acids, digest fats, and make nitric oxide. Nitric oxide helps keep blood vessels flexible, controls blood pressure, and protects against harmful cells and microbes.
When nitric oxide is low, undigested food particles build up in the small intestine and bloodstream, making it harder for cells to get oxygen and energy. This causes white blood cells, muscle cells, and platelets to work together to clear out damaged cells. This process forms clots, scar tissue, and new blood vessels, leading to a condition called atherosclerosis, which is linked to inflammation and harmful byproducts.

Figure 6: Atherosclerosis is when arteries thicken and harden from plaque buildup, which reduces blood flow and increases blood pressure. Over time, it causes inflammation and damages organs like the heart, pancreas, spleen, and legs, making them larger and less functional.
Autoimmune Disorders, Infections, and Cancers
Chronic hypernatremia (high sodium levels) disrupts the body’s energy use and fluid balance. It redirects blood towards important organs like the heart, brain, and muscles, and away from less critical organs such as the kidneys, skin, and digestive tract. This leads to a series of harmful reactions that damage organs and increase the risk of autoimmune diseases, infections, and cancers.
The liver begins to make more glucose from food and turns undigested food, especially proteins and fats, into stored fat, but it stops breaking down fat for energy. It also increases muscle breakdown and stores fat in blood vessels, organs, and tissues. These processes release reactive oxygen species (ROS) and pro-inflammatory proteins like cytokines.
The excess heat from ROS can oxidize cholesterol (especially LDL), which can then build up in injured blood vessel walls. White blood cells (macrophages) try to clear the excess cholesterol, causing inflammation and the thickening of blood vessels (atherosclerosis). This process damages cells, mutates genes, and slows down cell growth.
Overactive white blood cells can attack the body’s own tissue, leading to autoimmune disorders like Crohn’s disease, rheumatoid arthritis, and diabetes. These abnormal cells can also cooperate with damaged cells and microbes (viruses, bacteria, etc.) to clear out toxic materials and support the spread of infections and cancers.

Figure 7: Chronic dehydration and dysbiosis can dysregulate sodium blood levels and set the stage for atherosclerosis-induced vascular inflammation, infections, cancer, and multiorgan depletion. (1) Tumor cells and pathogens are recruited by platelets to ingest free hemin and iron, respectively, that are released by old and damaged cells in the circulation. This feeds these cells, which enables bugs and cancer cancers to reproduce and migrate. (2) Neutrophils stabilize the integrity and function of the blood vessel by releasing proinflammatory proteins and preventing natural killer (NK) cells from ingesting and destroying tumor cells and pathogens . (3) This enables tumor cells to activate platelets 39 and (4) support new blood vessel formation (angiogenesis) . (5 and 6) Thus, the cytokines released by white blood cells enable pathogens to produce toxins that damage red blood cell membranes, steal nutrients (like iron and oxygen) from other organs, and induce infections and tumor growth and migration, as well as prevent excessive bleeding 16.
High sodium levels can increase the risk and severity of various health problems, including metabolic, endocrine, and autoimmune disorders. These disorders can damage organs and lower quality of life. Conditions like rheumatoid arthritis (RA), lupus, inflammatory bowel disease (IBD), and multiple sclerosis are linked to an overactive immune response triggered by imbalanced fluid and electrolyte levels. A study of nearly 112,000 people found that RA patients had a 50% higher risk of death, similar to the risk seen in diabetics. Early detection and treatment of high sodium can help manage these health risks and prevent serious complications.
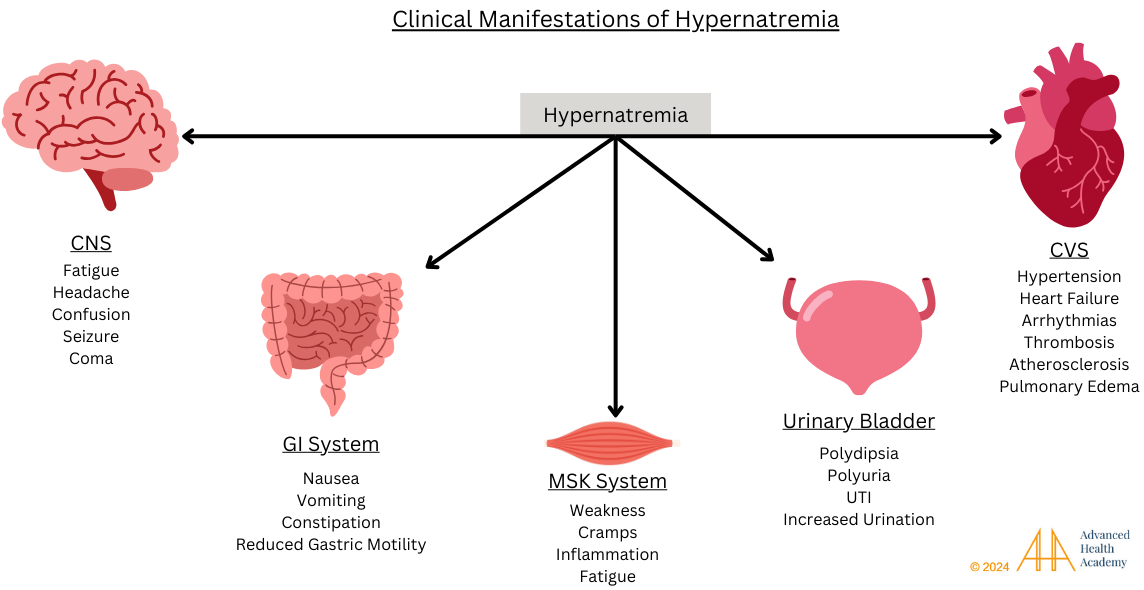
Figure 8: High sodium levels in the blood (hypernatremia) can damage organs and cause health issues. It affects fluid balance, blood pressure, muscle function, and brain activity. In the brain, it can cause confusion, seizures, or coma. In the digestive system, it can lead to nausea, vomiting, and constipation. Muscles can cramp or weaken from dehydration. In the urinary system, it may cause frequent urination and infections. For the heart, it can raise blood pressure and increase the risk of heart attack, stroke, and failure.
Clinical Significance of Low Blood Sodium Levels
Low blood sodium (hyponatremia) disrupts fluid balance and harms important cell functions. Sodium helps control the balance of body fluids and supports nerve signaling and muscle movement. When sodium levels drop too low, water moves into cells, causing them to swell. This swelling prevents cells from working properly. Chronic hyponatremia can affect all organs and interfere with essential processes that are necessary for life.
Reduced Bone Mineralization
Low sodium levels can affect other electrolytes like calcium, magnesium, and phosphate, which are important for bone health and energy production. Chronic low sodium (hyponatremia) can lead to weaker bones, balance problems, falls, fractures, and slower healing of wounds.
Joint and Muscle Pain
Hyponatremia, or low sodium, can worsen joint inflammation and thin cartilage, leading to joint pain, reduced movement (osteoarthritis), and a higher risk of tendon rupture. It can also impact muscle function, causing cramps, weakness, and in severe cases, muscle breakdown.
Brain and Nerve Damage
Hyponatremia, or low sodium, can cause brain swelling and affect how neurotransmitters are released. Neurotransmitters help nerve cells communicate and keep the brain working properly. Low sodium levels can damage the brain and nerves, leading to symptoms like headaches, confusion, brain swelling, coma, seizures, and even death.
Multi-Organ Damage
Low sodium in the blood can reduce blood flow to organs and lower blood pressure. When blood flow to the kidneys drops, the body releases antidiuretic hormone (ADH), causing the kidneys to keep more water and dilute sodium. This leads to hyponatremia, even if sodium levels seem normal. This is called the Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH). Adrenal insufficiency, where the body lacks hormones like aldosterone and cortisol, can also affect sodium balance. Without aldosterone, the kidneys lose more sodium, causing low blood pressure and other issues. SIADH symptoms include confusion, seizures, and muscle cramps. Low sodium from poor heart blood flow can cause fatigue, weakness, and trouble exercising.
Prevalence and Statistics of Abnormal Blood Sodium Levels
High or low blood sodium levels can strain organs like the heart, kidneys, and liver. A 2013 study showed that too much sodium worsens autoimmune diseases by increasing immune cells that attack the body. People with high sodium diets had 10 times more of these cells than those with low sodium diets. A 2015 study found that patients with fractures had lower sodium levels. Those with severe osteoporosis had even lower levels, especially older adults. Low sodium can increase the risk of fractures and death in hospitalized patients, and it can worsen conditions like heart failure and kidney disease.
Conclusion
Sodium is important for health because it helps balance fluids, regulate other electrolytes, and support functions like blood pressure, nerve activity, and muscle contractions. When sodium levels are too high or too low, it can cause problems like muscle cramps, heart issues, dizziness, joint pain, and more fractures. Abnormal sodium can also affect organs like the kidneys, heart, digestive system, and blood vessels. To manage sodium levels, it’s important to eat fewer processed foods and more plant-based items like vegetables and fruits. Staying hydrated, limiting alcohol, managing stress, and getting good sleep can also help keep sodium in balance. By maintaining proper sodium levels, we can prevent serious health problems like heart attack, stroke, kidney failure, and gut disorders.
Source References and Supplemental Research
Titze J. Sodium balance is not just a renal affair. Curr Opin Nephrol Hypertens. 2014;23(2):101-105. doi:10.1097/01.mnh.0000441151.55320.c3 [PubMed]
National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Food and Nutrition Board; Committee to Review the Dietary Reference Intakes for Sodium and Potassium; Oria M, Harrison M, Stallings VA, editors. Dietary Reference Intakes for Sodium and Potassium. Washington (DC): National Academies Press (US); 2019 Mar 5. 3, Methodological Considerations. Available from: [PubMed]
Pass the Salt: Sodium’s Role in Nerve Signaling and Stress on Blood Vessels. NIGMS Biomedical Beat Blog. [NIH]
Kuo IY, Ehrlich BE. Signaling in muscle contraction. Cold Spring Harb Perspect Biol. 2015;7(2):a006023. Published 2015 Feb 2. doi:10.1101/cshperspect.a006023 [PubMed]
Wein H. How the body regulates salt levels. National Institutes of Health (NIH). Published May 2017. [NIH]
Pirahanchi Y, Jessu R, Aeddula NR. Physiology, Sodium Potassium Pump. [Updated 2023 Mar 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: [NIH]
De Wardener HE, MacGregor GA. Sodium and blood pressure. Curr Opin Cardiol. 2002;17(4):360-367. doi:10.1097/00001573-200207000-00007 [PubMed] [Full Text]
de Wardener HE. The control of sodium excretion. Am J Physiol. 1978;235(3):F163-F173. doi:10.1152/ajprenal.1978.235.3.F163 [PubMed] [Full Text]
Scott JH, Menouar MA, Dunn RJ. Physiology, Aldosterone. [Updated 2023 May 1]. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: [PubMed]
Song W, Wang H, Wu Q. Atrial natriuretic peptide in cardiovascular biology and disease (NPPA). Gene. 2015;569(1):1-6. doi:10.1016/j.gene.2015.06.029 [PubMed]
Schweda F. Salt feedback on the renin-angiotensin-aldosterone system. Pflugers Arch. 2015;467(3):565-576. doi:10.1007/s00424-014-1668-y [PubMed] [Springer]
Ramsay DJ. Homeostatic control of water balance. In: Arnaud MJ, editor. Hydration Throughout Life. Montrouge: John Libbey Eurotext; 1998. pp. 9–18. [Google Scholar]
Chung J, Chen C, Paw BH. Heme metabolism and erythropoiesis. Curr Opin Hematol. 2012;19(3):156-162. doi:10.1097/MOH.0b013e328351c48b [PubMed] [Full Text] [PMC]
McClellan S, Walsh T. Oxygen delivery and hemoglobin. Contin Educ Anaesth Crit Care Pain 2004; 4: 123-26, [Full Text]
Hom J, Dulmovits BM, Mohandas N, Blanc L. The erythroblastic island as an emerging paradigm in the anemia of inflammation. Immunol Res. 2015;63(1-3):75-89. doi:10.1007/s12026-015-8697-2 [PubMed] [Springer]
Bunn HF. Hemoglobin I. Structure and function. In: Beck WS, Hematology. Cambridge, MA: MIT Press, 1981;129. [Research Gate]
Kastl AJ Jr, Terry NA, Wu GD, Albenberg LG.The Structure and Function of the Human Small Intestinal Microbiota: Current Understanding and Future Directions. [ScienceDirect]. Accessed July 21, 2024.
Reddy, S., Ramsubeik, K., Vega, K. J., Federico, J., & Palacio, C. (2010). Do HbA1C Levels Correlate With Delayed Gastric Emptying in Diabetic Patients?. Journal of neurogastroenterology and motility, 16(4), 414–417. [JNM] [Crosslink]
Abumrad NA, Davidson NO. Role of the gut in lipid homeostasis. Physiol Rev 2012; 92:1061-1085 [PMC free article] [PubMed]
Wu G. Amino acids: metabolism, functions, and nutrition. Amino Acids. 2009;37(1):1-17. doi:10.1007/s00726-009-0269-0 [Pubmed][Crossref]
Jakubowski H., Flatt P. Metabolic Fates of Amino Groups. LibreTexts Biology. [LibreTexts]
Liu, H., Huang, Y., Huang, M. et al. From nitrate to NO: potential effects of nitrate-reducing bacteria on systemic health and disease. Eur J Med Res 28, 425 (2023). https://doi.org/10.1186/s40001-023-01413-y [BMC]
Bryan, N.S., Petrosino, J.F. (2017). Nitrate-Reducing Oral Bacteria: Linking Oral and Systemic Health. In: Bryan, N., Loscalzo, J. (eds) Nitrite and Nitrate in Human Health and Disease. Nutrition and Health. Humana Press, Cham. https://doi.org/10.1007/978-3-319-46189-2_3 [Springer]
Song Y, Liu J, Zhao K, Gao L, Zhao J. Cholesterol-induced toxicity: An integrated view of the role of cholesterol in multiple diseases. Cell Metabolism. 2021;33(10):1911-1925. doi:10.1016/j.cmet.2021.09.001 [Elsevier]
Adiels M, Olofsson SO, Taskinen MR, Borén J. Overproduction of very low-density lipoproteins is the hallmark of the dyslipidemia in the metabolic syndrome. Arterioscler Thromb Vasc Biol. 2008;28(7):1225-1236. doi:10.1161/ATVBAHA.107.160192 [PubMed] [Full Text] [AHA Journals]
Rouyez MC, Boucheron C, Gisselbrecht S, Dusanter-Fourt I, Porteu F. Control of thrombopoietin-induced megakaryocytic differentiation by the mitogen-activated protein kinase pathway. Mol Cell Biol. 1997;17:4991-5000 [PubMed] [PMC Full Text]
Zhao. Platelet generation from circulating megakaryocytes is triggered in the lung vasculature. BioRXiv (2021) bioRxiv 2021.11.01.466743. doi: 10.21203/rs.3.rs-690639/v1 [BioRXiv Full Text] [Crosslink]
Gelon L, Fromont L, Lefrançais E. Occurrence and role of lung megakaryocytes in infection and inflammation. Frontiers in Immunology. 2022;13. doi:10.3389/fimmu.2022.1029223 [PubMed] [PMC Full Text] [Crosslink]
Poirault-Chassac S, Nivet-Antoine V, Houvert A, Kauskot A, Lauret E, Lai-Kuen R, et al. Mitochondrial dynamics and reactive oxygen species initiate thrombopoiesis from mature megakaryocytes. Blood Adv (2021) 5(6):1706–18. doi: 10.1182/bloodadvances.2020002847 [PubMed] [PMC Full Text] [Crosslink]
Wilson J.G., Lindquist J.H., Grambow S.C., Crook E.D., Maher J.F. Potential role of increased iron stores in diabetes. Am. J. Med. Sci. 2003;325:332–339. doi: 10.1097/00000441-200306000-00004. [PubMed] [CrossRef] [Google Scholar]
Tiedge M., Lortz S., Drinkgern J., Lenzen S. Relation between antioxidant enzyme gene expression and antioxidative defense status of insulin-producing cells. Diabetes. 1997;46:1733–1742. doi: 10.2337/diab.46.11.1733. [PubMed] [CrossRef] [Google Scholar]
Crawford JH, Chacko BK, Kevil CG, Patel RP. The red blood cell and vascular function in health and disease. Antioxidants & redox signaling. 2004;6(6):992–999. [PubMed] [Google Scholar]
Della Corte V, Todaro F, Cataldi M, Tuttolomondo A. Atherosclerosis and Its Related Laboratory Biomarkers. Int J Mol Sci. 2023;24(21):15546. Published 2023 Oct 24. doi:10.3390/ijms242115546 [PMC Full Text]
Michel JB, Martin-Ventura JL. Red Blood Cells and Hemoglobin in Human Atherosclerosis and Related Arterial Diseases. Int J Mol Sci. 2020;21(18):6756. Published 2020 Sep 15. doi:10.3390/ijms21186756 [PMC Full Text]
Dludla P.V., Joubert E., Muller C.J.F., Louw J., Johnson R. Hyperglycemia-induced oxidative stress and heart disease-cardioprotective effects of rooibos flavonoids and phenylpyruvic acid-2-O-beta-D-glucoside. Nutr. Metab. 2017;14:45. doi: 10.1186/s12986-017-0200-8. [PMC free article] [PubMed] [CrossRef] [Google Scholar].
Žiberna, L., Jenko-Pražnikar, Z., & Petelin, A. (2021). Serum Bilirubin Levels in Overweight and Obese Individuals: The Importance of Anti-Inflammatory and Antioxidant Responses. Antioxidants (Basel, Switzerland), 10(9), 1352. [PubMed] [MDPI] [PubMed] [Crosslink]
Chen, L., Deng, H., Cui, H., Fang, J., Zuo, Z., Deng, J., Li, Y., Wang, X., & Zhao, L. (2017). Inflammatory responses and inflammation-associated diseases in organs. Oncotarget, 9(6), 7204–7218. [Oncotarget] [Crosslink]
Setién-Suero E, Suárez-Pinilla M, Suárez-Pinilla P, Benedicto Crespo-Facorro, Ayesa-Arriola R. Homocysteine and cognition: A systematic review of 111 studies. 2016;69:280-298. doi:https://doi.org/10.1016/j.neubiorev.2016.08.014 [Elsevier]
Perna AF, Ingrosso D. Atherosclerosis determinants in renal disease: how much is homocysteine involved?. Nephrol Dial Transplant. 2016;31(6):860-863. doi:10.1093/ndt/gfv409 [PubMed] [Oxford Academic]
Schaffer A, Verdoia M, Cassetti E, et al. Relationship between homocysteine and coronary artery disease. Results from a large prospective cohort study. Thromb Res. 2014;134(2):288-293. doi:10.1016/j.thromres.2014.05.025 [PubMed] [Elsevier]
Emanuelsson, F., Nordestgaard, B. G., & Benn, M. (2018). Familial hypercholesterolemia and risk of peripheral arterial disease and chronic kidney disease. The Journal of Clinical Endocrinology & Metabolism, 103(12), 4491–4500. https://doi.org/10.1210/jc.2018-01058 [CrossRef] [Google Scholar] [Scopus]
Conigliaro, P., Chimenti, Triggianese, P., Sunzini, F., Novelli, L., Perricone, C., & Perricone, R. (2016). Autoantibodies in inflammatory arthritis. Autoimmunity Reviews, 15(7), 673–683. https://doi.org/10.1016/j.autrev.2016.03.003 [Science Direct]
Feingold, K. R., & Grunfeld, C. (2022, March 7). The effect of inflammation and infection on lipids and lipoproteins. Endotext – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK326741/ [NIH]
Mrabet, S., Wafa, M., & Giovannoni, G. (2022). Multiple sclerosis and migraine: Links, management and implications. Multiple Sclerosis and Related Disorders, 68, 104152. https://doi.org/10.1016/j.msard.2022.104152 [Science Direct]
Avina-Zubieta JA, Choi HK, Sadatsafavi M, Etminan M, Esdaile JM, Lacaille D. Risk of cardiovascular mortality in patients with rheumatoid arthritis: a meta-analysis of observational studies. Arthritis Rheum. 2008;59:1690–1697. [PubMed] [Reference list]
Lindhardsen J, Ahlehoff O, Gislason GH, Madsen OR, Olesen JB, Torp-Pedersen C, Hansen PR. The risk of myocardial infarction in rheumatoid arthritis and diabetes mellitus: a Danish nationwide cohort study. Ann Rheum Dis. 2011;70:929–934. [PubMed] [Reference list]
Verbalis JG, Barsony J, Sugimura Y, et al. Hyponatremia-induced osteoporosis. J Bone Miner Res. 2010;25(3):554-563. doi:10.1359/jbmr.090827 [PubMed]
Achmad A, Suharjono, Soeroso J, et al. The sodium does not affect joint pain and functional activity of knee osteoarthritis patients. J Public Health Afr. 2023;14(Suppl 1):2494. Published 2023 Mar 16. doi:10.4081/jphia.2023.2494.[PubMed]
Mathew DM, Chilakala A, Elfert K. Rhabdomyolysis in the Setting of Severe Hyponatremia: A Case Report. Cureus. 2023;15(6):e39993. Published 2023 Jun 5. doi:10.7759/cureus.39993 [PubMed]
Giuliani C, Peri A. Effects of Hyponatremia on the Brain. J Clin Med. 2014;3(4):1163-1177. Published 2014 Oct 28. doi:10.3390/jcm3041163 [PubMed]
Rodriguez M, Hernandez M, Cheungpasitporn W, et al. Hyponatremia in Heart Failure: Pathogenesis and Management. Curr Cardiol Rev. 2019;15(4):252-261. doi:10.2174/1573403X15666190306111812 [PubMed]
Yasir M, Mechanic OJ. Syndrome of Inappropriate Antidiuretic Hormone Secretion. [Updated 2023 Mar 6]. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024 Jan.
Jessani N, Jehangir W, Behman D, Yousif A, Spiler IJ. Secondary adrenal insufficiency: an overlooked cause of hyponatremia. J Clin Med Res. 2015;7(4):286-288. doi:10.14740/jocmr2041w [PubMed]
Shanthosh Kumar S, Nagesh VK, Hunter J, Sange I. A Case of Severe Hyponatremia in a Patient With Primary Adrenal Insufficiency. Cureus. 2021;13(9):e17946. Published 2021 Sep 13. doi:10.7759/cureus.17946 [PubMed]
Borrelli S, Provenzano M, Gagliardi I, et al. Sodium Intake and Chronic Kidney Disease. Int J Mol Sci. 2020;21(13):4744. Published 2020 Jul 3. doi:10.3390/ijms21134744 [PubMed]
Yale School of Medicine. (2013, May 31). Salt is new culprit in autoimmunity. Yale School of Medicine. [Yale Medicine].
Kwak MK, Choi D, Lee JH, et al. Relationship between Decrease in Serum Sodium Level and Bone Mineral Density in Osteoporotic Fracture Patients. J Bone Metab. 2015;22(1):9-15. doi:10.11005/jbm.2015.22.1.9 [PubMed]
Chawla A, Sterns RH, Nigwekar SU, Cappuccio JD. Mortality and serum sodium: do patients die from or with hyponatremia?. Clin J Am Soc Nephrol. 2011;6(5):960-965. doi:10.2215/CJN.10101110 [PubMed]
Committee on the Consequences of Sodium Reduction in Populations; Food and Nutrition Board; Board on Population Health and Public Health Practice; Institute of Medicine; Strom BL, Yaktine AL, Oria M, editors. Sodium Intake in Populations: Assessment of Evidence. Washington (DC): National Academies Press (US); 2013 Aug 27. 4, Sodium Intake and Health Outcomes. Available from: [PubMed]
Chrysant SG. Effects of High Salt Intake on Blood Pressure and Cardiovascular Disease: The Role of COX Inhibitors. Clin Cardiol. 2016;39(4):240-242. https://doi.org/10.1002/clc.22536 [Wiley]
Lower sodium could reduce blood pressure in most people. National Institutes of Health (NIH). Published December 4, 2023. [NIH]
Shi H, Su X, Li C, Guo W, Wang L. Effect of a low-salt diet on chronic kidney disease outcomes: a systematic review and meta-analysis. BMJ Open. 2022;12(1):e050843. Published 2022 Jan 11. doi:10.1136/bmjopen-2021-050843 [PubMed]
Gai, Z., Wang, T., Visentin, M., Kullak-Ublick, G., Fu, X., & Wang, Z. (2019). Lipid accumulation and chronic kidney disease. Nutrients, 11(4), 722. https://doi.org/10.3390/nu11040722 [PubMed]
Lee, S., & Ho, K. (1978). Cholesterol fatty kidney: Morphological changes in the course of its development in rabbits. Experimental and Molecular Pathology, 29(3), 412–425. https://doi.org/10.1016/0014-4800(78)90082-5 [ScienceDirect]
Liang, X., Ye, M., Tao, M., Zheng, D., Cai, R., Zhu, Y., Jin, J., & He, Q. (2020). The association between dyslipidemia and the incidence of chronic kidney disease in the general Zhejiang population: a retrospective study. BMC Nephrology, 21(1). https://doi.org/10.1186/s12882-020-01907-5 [PubMed]
Little R, Ellison DH. Modifying Dietary Sodium and Potassium Intake: An End to the ‘Salt Wars’?. Hypertension. 2024;81(3):415-425. doi:10.1161/HYPERTENSIONAHA.123.19487 [PubMed] [Full Text]
Zarantonello D, Brunori G. The Role of Plant-Based Diets in Preventing and Mitigating Chronic Kidney Disease: More Light than Shadows. J Clin Med. 2023;12(19):6137. Published 2023 Sep 22. doi:10.3390/jcm12196137 [PubMed]
Jardine MA, Kahleova H, Levin SM, Ali Z, Trapp CB, Barnard ND. Perspective: Plant-Based Eating Pattern for Type 2 Diabetes Prevention and Treatment: Efficacy, Mechanisms, and Practical Considerations. Adv Nutr. 2021;12(6):2045-2055. doi:10.1093/advances/nmab063 [PubMed]
Dundas B, Harris M, Narasimhan M. Psychogenic polydipsia review: etiology, differential, and treatment. Curr Psychiatry Rep. 2007;9(3):236-241. doi:10.1007/s11920-007-0025-7 [PubMed]
Kennedy M. How much water you’re actually supposed to drink each day – and why 8 cups isn’t right for everyone. Business Insider. December 14, 2021. [Website]
Veniamakis E, Kaplanis G, Voulgaris P, Nikolaidis PT. Effects of Sodium Intake on Health and Performance in Endurance and Ultra-Endurance Sports. Int J Environ Res Public Health. 2022;19(6):3651. Published 2022 Mar 19. doi:10.3390/ijerph19063651 [PubMed]
Dmitrieva NI, Burg MB. Elevated sodium and dehydration stimulate inflammatory signaling in endothelial cells and promote atherosclerosis. PLoS One. 2015;10(6):e0128870. Published 2015 Jun 4. doi:10.1371/journal.pone.0128870 [PubMed]
Sterns RH, Thomas DJ, Herndon RM. Brain dehydration and neurologic deterioration after rapid correction of hyponatremia. Kidney Int. 1989;35(1):69-75. doi:10.1038/ki.1989.9 [PubMed]
Khan S, Floris M, Pani A, Rosner MH. Sodium and Volume Disorders in Advanced Chronic Kidney Disease. Adv Chronic Kidney Dis. 2016;23(4):240-246. doi:10.1053/j.ackd.2015.12.003 [PubMed] [Elsevier]
Jiang X, Anasanti MD, Drenos F, Blakemore AI, Pazoki R. Urinary Sodium Excretion Enhances the Effect of Alcohol on Blood Pressure. Healthcare (Basel). 2022;10(7):1296. Published 2022 Jul 13. doi:10.3390/healthcare10071296 [PubMed]
Markiewicz K, Chmura J, Cholewa M. Wpływ palenia papierosów na steźenie sodu, potasu i chloru we krwi oraz na niektóre parametry równowagi kwasowo-zasadowej w czasie wysiłku fizycznego i restytucji [Effect of tobacco smoking on plasma sodium, potassium and chloride concentrations and some parameters of acid-base equilibrium during physical exertion and in the course of restitution]. Med Pr. 1977;28(6):473-480. [PubMed]
Lee J, Taneja V, Vassallo R. Cigarette smoking and inflammation: cellular and molecular mechanisms. J Dent Res. 2012;91(2):142-149. doi:10.1177/0022034511421200 [PubMed]
Oakes JM, Fuchs RM, Gardner JD, Lazartigues E, Yue X. Nicotine and the renin-angiotensin system. Am J Physiol Regul Integr Comp Physiol. 2018;315(5):R895-R906. doi:10.1152/ajpregu.00099.2018 [PubMed]
Liamis G, Milionis H, Elisaf M. A review of drug-induced hyponatremia. Am J Kidney Dis. 2008;52(1):144-153. doi:10.1053/j.ajkd.2008.03.004 [PubMed] [Elsevier]
Ray EC, Rondon-Berrios H, Boyd CR, Kleyman TR. Sodium Retention and Volume Expansion in Nephrotic Syndrome: Implications for Hypertension. Advances in Chronic Kidney Disease. 2015;22(3):179-184. doi:https://doi.org/10.1053/j.ackd.2014.11.006 [Elsevier]
Ge D, Su S, Zhu H, et al. Stress-induced sodium excretion: a new intermediate phenotype to study the early genetic etiology of hypertension?. Hypertension. 2009;53(2):262-269. doi:10.1161/HYPERTENSIONAHA.108.118117 [PubMed]
Torres SJ, Turner AI, Nowson CA. Does stress induce salt intake? British Journal of Nutrition. 2010;103(11):1562-1568. doi:10.1017/S000711451000098X [Cambridge]
Knutson KL. Impact of sleep and sleep loss on glucose homeostasis and appetite regulation. Sleep Med Clin. 2007;2(2):187-197. doi:10.1016/j.jsmc.2007.03.004 [PubMed]
Hirshkowitz M, Whiton K, Albert SM, et al. National Sleep Foundation’s sleep time duration recommendations: methodology and results summary. Sleep Health. 2015;1(1):40-43. doi:10.1016/j.sleh.2014.12.010 [PubMed] [Elsevier]
Hamasaki H. The Effects of Mindfulness on Glycemic Control in People with Diabetes: An Overview of Systematic Reviews and Meta-Analyses. Medicines (Basel). 2023;10(9):53. Published 2023 Sep 7. doi:10.3390/medicines10090053 [PubMed]
Pascoe MC, Thompson DR, Jenkins ZM, Ski CF. Mindfulness mediates the physiological markers of stress: Systematic review and meta-analysis. J Psychiatr Res. 2017;95:156-178. doi:10.1016/j.jpsychires.2017.08.004 [PubMed] [Elsevier]